







Evaluation of Intra-Fractional Target Position Variation during Deep Inspiration Breath-Hold (DIBH) Sessions in Lung Stereotactic Body Radiotherapy (SBRT)
Abstract
Introduction: The integration of Deep Inspiration Breath Hold (DIBH) in lung Stereotactic Body Radiation Therapy (SBRT), coupled with optical imaging modalities, enhances the consistency of target localization and reduces healthy tissue toxicity. However, variability between DIBH sessions may lead to target misalignment, potentially impacting treatment outcomes. The purpose of this study was to evaluate intra-fractional target position variation during DIBH in lung SBRT, reflecting the combined effects of intra-fractional motion and inter-breath-hold variability.
Methodology: A retrospective analysis of 14 patients treated between 2021 and 2023 was conducted. Intra-fractional target position variation during DIBH was quantified using intra-fraction CBCT couch-shift records, with 111 DIBH pairs analyzed. Dosimetric impacts were calculated by applying couch shifts to original plans’ isocenters.
Results: Ten out of 14 patients (71%) had DIBH variation of <5 mm in all directions, with average variations of -0.68 mm ±1.90 mm vertically, -1.26 mm ±3.53 mm longitudinally, and -0.24 mm ±1.43 mm laterally. The remaining four patients exhibited >5 mm target shifts between DIBH sessions. Worst-case scenario dose computations indicated reductions in GTV receiving 100% of the prescription dose (V100%) ranging from -9.48% to -100%. A simulated delivery study for the patient with the largest DIBH variations showed an average GTV V100% coverage decrease from 99.91% to 70.57% (SD 13%).
Conclusion: Although many patients can achieve DIBH with <5 mm variation, the large target position variation during DIBH observed in this study underscores the need for improved patient screening, DIBH coaching, and practice to ensure a successful DIBH treatment.
Keywords: DIBH, Lung SBRT, Intra-fraction motion, CBCT, Target localization.
Introduction
Ensuring accurate target localization in radiation therapy for lung cancer patients remains a significant challenge due to uncertainties arising from respiratory motion1. This underscores the necessity of implementing effective motion management strategies to ensure precise treatment delivery1. Various motion management techniques have been developed to reduce the impact of respiratory motion during radiation therapy, including breath-hold techniques, respiratory gating, and tumor tracking1. The effectiveness of these approaches depends heavily on the consistency and reproducibility of the patient’s breathing pattern, as greater regularity enhances the reliability of motion management and target alignment1.
The integration of Deep Inspiration Breath Hold (DIBH) into lung Stereotactic Body Radiation Therapy (SBRT), particularly when combined with optical imaging modalities, has demonstrated improvements in target localization reproducibility, reduction in treatment margins, and decreased radiation exposure to healthy surrounding tissues2,3. Mørkeset et al3 suggested that modern technological advancements and refined clinical workflows facilitate effective implementation of DIBH, demonstrating high patient compliance in lung SBRT. Furthermore, the use of DIBH during CBCT image acquisition has been shown to improve image quality due to reduced respiratory motion during breath-hold, thereby enhancing registration accuracy, particularly in the craniocaudal direction, and improving the precision of Image-Guided Radiation Therapy (IGRT) for lung cancer patients4.
Respiratory motion is a complex and largely subconscious physiological process, primarily driven by diaphragmatic movement. It presents a significant challenge to accurate radiation delivery in thoracic malignancies. Recent studies have highlighted the feasibility and efficacy of Surface-Guided Radiation Therapy (SGRT) when combined with IGRT during DIBH for lung cancer patients5,6,7. This integrated approach has been shown to be clinically feasible and straightforward to implement.5 Moreover, SGRT has demonstrated reliability as a surrogate for internal target motion, providing valuable information for patient setup verification and intra-fraction motion monitoring6,7.
In lung SBRT, inter-fractional errors are typically mitigated through daily image guidance. However, intra-fractional variations remain a greater concern, requiring precise measurement and quantification to ensure accurate target localization and dose delivery8. Although DIBH significantly reduces respiratory-induced motion, complete elimination of intra-fractional variation is challenging due to breath-hold reproducibility limitations and physiological factors such as cardiac-induced tumor motion8. Additionally, patient-specific and treatment-related factors—including treatment duration, respiratory excursion, and immobilization techniques—may further contribute to intra-fractional target position variability during lung SBRT9.
Several studies have investigated lung tumor motion management, with findings indicating that structured patient coaching combined with visually guided DIBH techniques can significantly reduce, though not entirely eliminate, tumor motion10,11,12,13,14. Nevertheless, successful implementation of DIBH depends strongly on patient compliance and consistency. Coaching has been proposed as an effective strategy to improve breath-hold reproducibility, promote sustainable breathing patterns, and distinguish between abdominal and thoracic breathing.11 Josipovic et al.12 reported that, following patient coaching, the median of the maximal tumor position deviations between consecutive DIBHs ranged from 0.9 to 1.3 mm. Additionally, visually guided breath-hold techniques have demonstrated intra-fraction reproducibility of less than 3 mm in lung SBRT13. Despite these promising results, the availability of structured coaching in routine clinical practice may vary, potentially affecting consistent implementation.
In summary, accurate DIBH treatment delivery relies on the reproducibility of consecutive breath-holds. Variability between DIBH sessions may introduce target misalignment during both imaging and treatment, potentially affecting dosimetric accuracy and clinical outcomes.
Despite its clinical importance, the consistency of target positioning during consecutive DIBH sessions under routine treatment conditions remains insufficiently characterized.
Therefore, this study aims to evaluate intra-fractional target position variation during DIBH in lung SBRT patients, reflecting the combined effects of intra-fractional motion and inter-breath-hold variability. Using intra-fractional CBCT data acquired during treatment delivery, this work seeks to quantify target position variation between consecutive DIBH sessions and assess their potential dosimetric implications.
Methodology
Within the context of DIBH setup, in addition to conventional intra- and inter-fractional motion, an additional component of uncertainty exists: inter-breath-hold motion, referring to the variation in target position between consecutive breath-holds within the same treatment fraction. During a single treatment fraction—or even within a single treatment field—patients may be required to perform multiple breath-holds. Clinically, patients typically perform initial breath-holds for IGRT, after which couch shifts are applied to align the target to the planned position, and treatment delivery begins. Given the requirement for multiple treatment fields and breath-holds per fraction, clinicians often rely on external body surface monitoring as a surrogate for internal target localization. Variability in breath-hold consistency may introduce discrepancies between external and internal target positioning.
Institutional Image Guidance Protocol
The imaging-guidance protocol implemented at the authors’ institution requires a minimum of two CBCT acquisitions for all patients undergoing lung SBRT with DIBH. The first CBCT, acquired at the beginning of each treatment fraction, is used to align the target to its planned position. CBCT registration was performed using soft tissue alignment to the target (GTV) with manual adjustment as needed. Patient positioning corrections were performed using a six-degree-of-freedom (6DoF) robotic couch (Varian Medical Systems); however, only translational couch shifts were applied and included in the analysis, while rotational corrections were not evaluated. A second CBCT is obtained mid-treatment, typically prior to the second arc in a dual-arc VMAT plan or before the fourth field in a six-field static IMRT plan, to evaluate intra-fractional target positioning.
Positional differences between CBCT1 and CBCT2 were interpreted as a surrogate measure of intra-fraction inter-breath-hold target position variability under clinical DIBH conditions. Because image registration was performed using soft tissue alignment to the target (GTV), tumor motion during individual breath-holds was expected to be minimized within the predefined gating window. However, because each CBCT acquisition required multiple breath-hold attempts, the measured differences may also reflect compounded variability arising both within and between CBCT acquisitions.
All treatments were delivered on a conventional C-arm linear accelerator (Varian Novalis Tx, Varian Medical Systems, Palo Alto, CA). CBCT acquisition time varied depending on the patient’s ability to maintain breath-hold within the designated gating window. For a typical DIBH CBCT scan, patients were required to perform multiple breath-holds (approximately 2–5) to complete the full acquisition, which generally took around 2–5 minutes. Since each CBCT acquisition required multiple DIBH attempts, the reconstructed CBCT represented an average anatomical state across several breath-holds rather than a single continuous breath-hold. Therefore, some degree of intra-CBCT anatomical variability may have been inherently incorporated into the acquired images. Breath-holds were performed under the guidance of the Real-time Position Management (RPM) system (Varian Medical Systems, Palo Alto, CA), an external respiratory monitoring system that tracks a marker block placed on the patient’s thoracoabdominal surface. The system provides real-time feedback and enables patients to maintain breath-holds within a predefined gating window to promote consistent breath-hold performance. Although CBCT-based alignment is performed during a specific breath-hold, subsequent treatment delivery relies on maintaining consistency within the predefined RPM gating window, which serves as a surrogate for internal target localization. All CBCT images and corresponding couch shifts were recorded in ARIA (v16.1, Varian Medical Systems) and retrospectively extracted for quantitative analysis of DIBH variation.
Data Collection
A retrospective analysis was conducted on treatment records from 14 patients treated at the authors’ institution between 2021 and 2023. Patient demographics and treatment characteristics are summarized in Table 1. The cohort included patients with primary or oligometastatic lung cancer who underwent DIBH-based SBRT. The study population consisted of four male and ten female patients, with ages ranging from 60 to 91 years. Planning target volume (PTV) sizes ranged from 3.09 cm3 to 74.04 cm3. Prescription doses ranged from 48 Gy to 60 Gy, delivered in 4 to 8 fractions. Treatment techniques included VMAT and static IMRT, as indicated in Table 1. This study was approved by the Institutional Review Board (IRB) at the authors’ institution.
Table 1. Patient characteristics
| Gender | Age | Treatment Site | Target Volume (cc) | Prescription (Gy/#fractions) | Plan Technique | |
|---|---|---|---|---|---|---|
| Patient 1 | Female | 91 | RLL Lung | 74.04 | 50 in 5 | Static IMRT |
| Patient 2 | Female | 70 | RLL Lung | Oct-36 | 50 in 5 | VMAT |
| Patient 3 | Male | 82 | LLL Lung | 14.32 | 50 in 5 | VMAT |
| RLL Lung | 33.77 | 50 in 5 | VMAT | |||
| Patient 4 | Female | 70 | RLL Lung | 26.67 | 50 in 5 | VMAT |
| RLL Lung | 11-Jan | 50 in 5 | VMAT | |||
| Patient 5 | Female | 69 | LLL Lung | 17.16 | 50 in 5 | VMAT |
| Patient 6 | Female | 80 | RUL Lung | 18.88 | 50 in 5 | VMAT |
| Patient 7 | Female | 72 | LLL Lung | 30.57 | 50 in 5 | VMAT |
| Patient 8 | Female | 70 | LLL Lung | Mar-98 | 48 in 4 | Static IMRT |
| RLL Lung, LLL Lung | 3.09, 6.78 | 60 in 8 | VMAT | |||
| Patient 9 | Male | 79 | RML Lung | Jun-76 | 50 in 5 | VMAT |
| Patient 10 | Male | 88 | RLL Lung | 66.48 | 50 in 5 | VMAT |
| Patient 11 | Female | 68 | LLL Lung | 8.21, 5.20 | 50 in 5 | VMAT |
| RLL Lung | 13.53, 8.94 | 50 in 5 | VMAT | |||
| Patient 12 | Male | 74 | LLL Lung | Sep-55 | 50 in 5 | VMAT |
| Patient 13 | Female | 64 | LLL Lung | May-33 | 50 in 5 | VMAT |
| LLL Lung | 13.35 | 50 in 5 | VMAT | |||
| Patient 14 | Female | 67 | LLL Lung, LUL Lung | 34.20, 26.75 | 50 in 5 | VMAT |
All patients were monitored during DIBH using the Real-time Position Management (RPM) system (Varian Medical Systems, Palo Alto, CA), with a predefined gating window of 5 mm centered on the average breath-hold level. The gating window was defined relative to the patient-specific baseline respiratory signal. Prior to simulation, patients underwent brief coaching, during which they were instructed to perform three consecutive breath-holds and to inhale a consistent volume of air for each DIBH, producing a stable amplitude on the RPM breathing trace. During both simulation and treatment, patients were guided to maintain breath-holds within the gating window and to achieve consistent chest wall elevation, with a minimum breath-hold duration of 20 seconds used as a criterion for DIBH suitability.
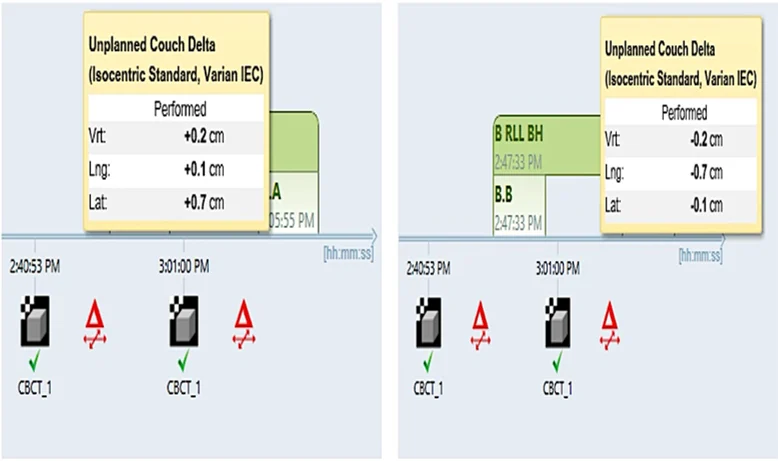
As described above, the initial couch shift within each fraction corrected setup uncertainty, whereas any subsequent couch shift primarily reflected intra-fractional patient motion and inter-breath-hold target displacement (DIBH variation). These DIBH variations were extracted from ARIA for further analysis (Figure 1). Descriptive statistical analysis was performed, including calculation of mean values and standard deviations, consistent with the exploratory nature of the study.
Figure 1. Pre-treatment (left) and intra-fractional (right) couch shifts. The second couch shift represents the DIBH-related target position variation.
Evaluation of Dosimetric Impact and Simulated Delivery Analysis
To assess the clinical significance of observed DIBH variations, dosimetric analyses were performed using Eclipse treatment planning system (v16.1, Varian Medical Systems, Palo Alto, CA) with the Acuros XB dose calculation algorithm.
Four of the 14 patients exhibited DIBH variations exceeding 5 mm and were selected for worst-case scenario dose evaluation. A threshold of 5 mm was used to define clinically significant variation, based on commonly reported planning target volume (PTV) margins in lung SBRT for motion-managed treatments. For each of these patients, dose recalculation was performed by shifting the planned isocenter by the maximum observed DIBH variation while maintaining the original fluence maps and monitor units. This approach simulated a scenario in which the maximum displacement persisted throughout treatment delivery.
To further evaluate cumulative effects under a more realistic clinical scenario in which DIBH variation may fluctuate across fractions, a simulated delivery study was performed for patient #3, who demonstrated the largest and most frequent DIBH variations across the five-fraction course. Ten simulated delivery scenarios were generated by randomly sampling observed DIBH variation magnitudes for each treatment field. For each simulation, the isocenter of the original plan was displaced according to the sampled variation, and a composite delivered dose distribution was generated. Dose metrics were extracted from the simulated delivery dose for statistical analysis. Evaluated parameters included the volumes of GTV and PTV receiving 100% of the prescription dose (GTV V100% and PTV V100%). These metrics were selected to quantify the impact of DIBH variation on target coverage.
Results
Across 120 treatment sessions involving 14 patients, a total of 222 intra-fractional CBCT scans were acquired, resulting in 111 measurable intra-fraction couch shifts. These couch shifts were recorded after correction of initial setup uncertainty and therefore primarily reflect residual intra-fraction positional variation during DIBH. Instances of 0 mm couch shifts were included in the analysis. In certain treatment sessions, additional intra-fraction CBCT scans were not acquired, for logistical or clinical reasons, accounting for the discrepancy between the number of treatment fractions and the total number of measured DIBH variations.
The distribution of DIBH variation across the three cardinal directions is illustrated in Figure 2. Among the three axes, longitudinal motion was the predominant direction of variation. Thirteen of the 111 DIBH variations (11.71%) exhibited longitudinal shifts exceeding 5 mm. In contrast, variations along the vertical and lateral directions were minimal. Only one vertical shift (0.90%) exceeded 5 mm; this occurred concurrently with a substantial longitudinal shift as well. No isolated lateral shifts greater than 5 mm were observed.
Figure 2. Distribution of DIBH-related target position variation across vertical, longitudinal, and lateral directions
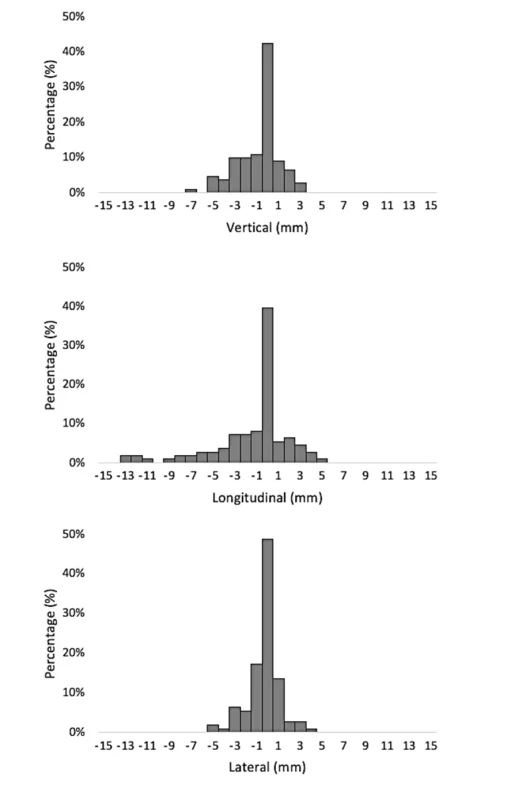
Descriptive analysis of DIBH variation showed mean shifts of −1.26 mm (SD 3.53 mm) in the longitudinal direction, −0.68 mm (SD 1.90 mm) in the vertical direction, and −0.24 mm (SD 1.43 mm) in the lateral direction. Variations exceeding 5 mm were observed in 13 of 111 cases (11.7%) in the longitudinal direction, with only one occurrence in the vertical direction and none in the lateral direction.
An additional observation was that DIBH variations were generally skewed toward negative values (Figure 2). In the superior-inferior axis, a negative shift indicates that the couch was moved inferiorly relative to the gantry to align with the reference CT image, implying that the target was positioned more superiorly in the subsequent CBCT compared to the initial scan.
From a population perspective, DIBH variations exceeding 5 mm were observed in four of the 14 patients (28.6%). For these four patients, worst-case scenario dose recalculations were performed under the assumption that the maximum observed DIBH variation persisted throughout treatment delivery. The resulting dose metrics are presented in Table 2.
Table 2. Worst-case scenario (WCS) dose computation results for patients with DIBH variation > 5 mm
| GTV V100% (Planned) | GTV V100% (WCS) | Reduction in GTV V100% | |
|---|---|---|---|
| Patient No.2 | 100.00% | 90.52% | -9.48% |
| Patient No.3 | 99.91% | 73.91% | -26.00% |
| Patient No.5 | 100.00% | 84.33% | -15.67% |
| Patient No.13 | 100.00% | 0.00% | -100.00% |
Reductions in GTV V100% ranged from -9.48% to -100%. Notably, patient #13 demonstrated a complete loss of GTV coverage in the worst-case scenario, as the magnitude of DIBH variation exceeded the dimension of the target volume (Figure 3).
Figure 3. Comparison of planned and worst-case scenario dose distributions for patient #13, demonstrating complete target miss due to DIBH variation exceeding target dimensions
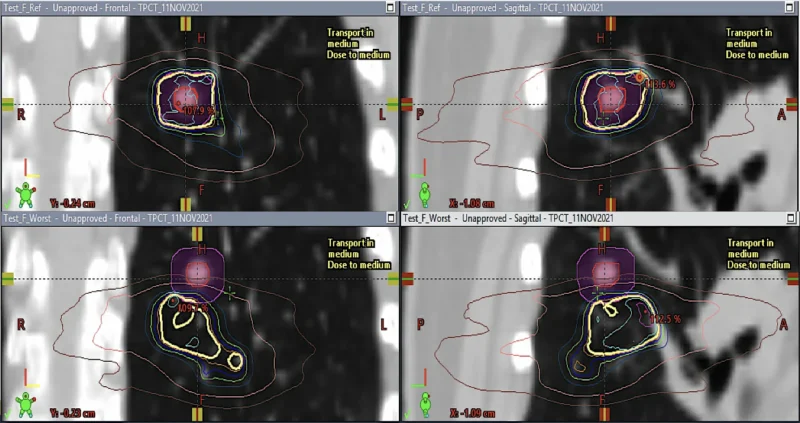
*The top panels show the planned dose distribution (coronal and sagittal views), while the bottom panels show the simulated worst-case distribution.
Patient #3 demonstrated the most frequent and largest DIBH variations. For this patient, simulated delivery analyses were conducted to evaluate the cumulative dosimetric impact of variable target position during DIBH. The results are summarized in Table 3.
Table 3. Simulated delivery dose metrics for Patient #3
Planned values: GTV V100% = 99.91%, GTV V95% = 100.00%, PTV V100% = 95.00%, PTV V95% = 99.98%.
| Scenario | GTV V100% | GTV V95% | PTV V100% | PTV V95% |
|---|---|---|---|---|
| 1 | 80.86% | 86.12% | 50.11% | 60.81% |
| 2 | 75.68% | 86.02% | 45.03% | 60.51% |
| 3 | 82.28% | 89.05% | 52.08% | 65.05% |
| 4 | 42.80% | 70.38% | 35.49% | 50.10% |
| 5 | 67.09% | 81.91% | 48.04% | 56.72% |
| 6 | 59.67% | 85.34% | 41.86% | 59.99% |
| 7 | 63.64% | 78.50% | 46.53% | 55.31% |
| 8 | 70.20% | 86.53% | 48.23% | 62.35% |
| 9 | 80.92% | 87.10% | 52.87% | 62.40% |
| 10 | 82.60% | 88.52% | 48.34% | 61.78% |
| Mean (SD) | 70.57% (13%) | 83.95% (6%) | 46.86% (5%) | 59.50% (-4%) |
Compared to the original plan (Figure 4), the mean GTV V100% decreased from 99.91% to 70.57% (SD 13%), and mean GTV V95% decreased from 100.00% to 83.95% (SD 6%).
Figure 4. Comparison of planned and simulated delivery target coverage metrics (GTV and PTV) for patient #3, showing the range and mean values across simulated scenarios
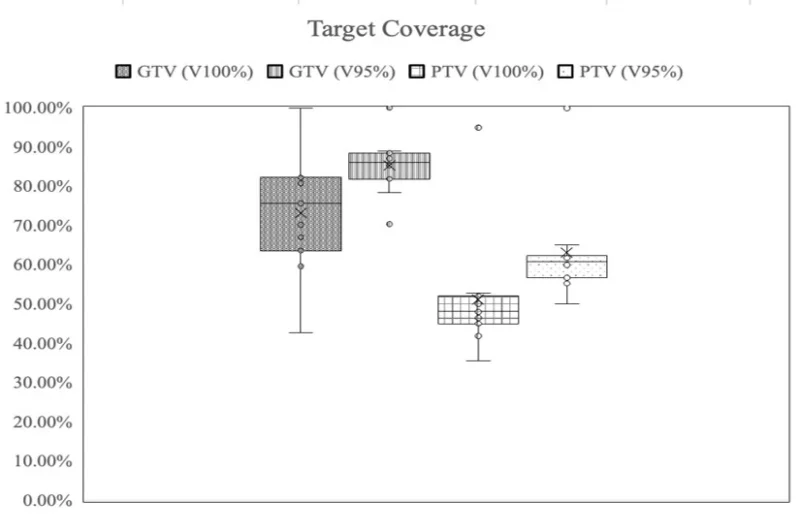
Similarly, mean PTV V100% decreased from 95.00% to 46.86% (SD 5%), and mean PTV V95% decreased from 99.98% to 59.50% (SD 4%). Figure 5 illustrates a representative comparison between the planned dose distribution and one simulated delivered dose distribution for patient #3.
Figure 5. Comparison of planned and simulated delivered dose distributions for patient #3
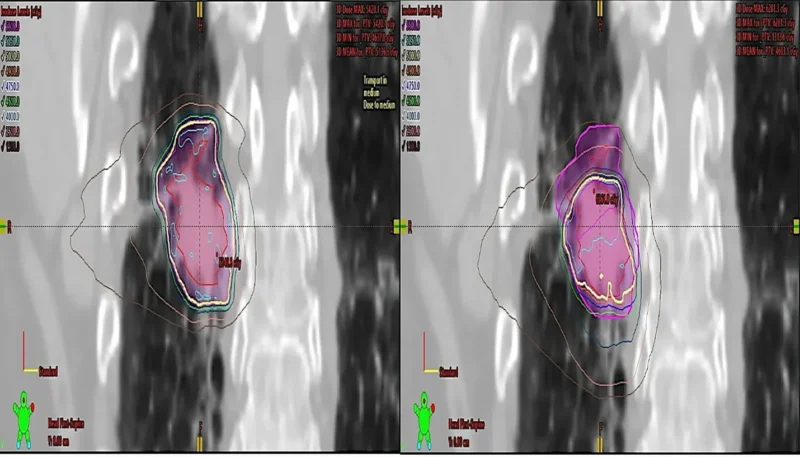
*The left panel shows the planned dose distribution, while the right panel shows a representative simulated delivered distribution.
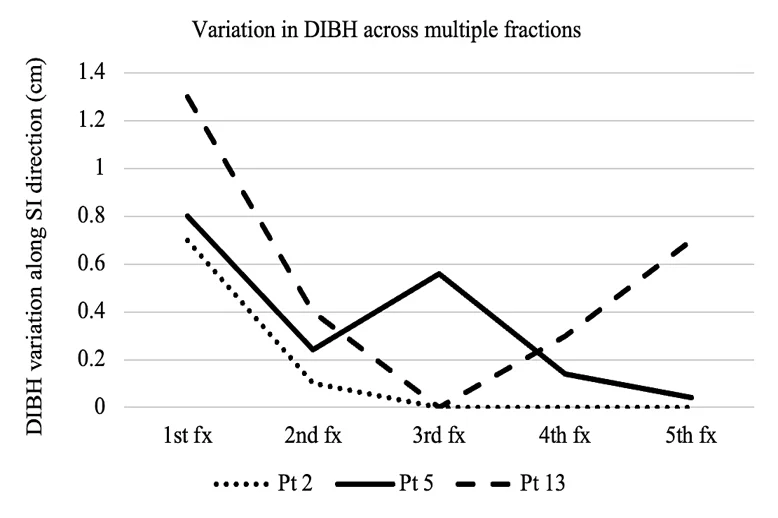
An additional observation was the trend toward reduced DIBH variation across treatment fractions in patients who initially demonstrated larger displacements. DIBH variations in the longitudinal direction, across treatment fractions, are plotted in Figure 6.
Figure 6. Longitudinal DIBH-related target position variation across treatment fractions in patients with initially large displacements, demonstrating a trend toward improved consistency over time
Discussion
This study evaluated intra-fractional target position variation during DIBH in lung SBRT using intra-fractional CBCT-derived couch shifts and quantified the dosimetric consequences of observed inter-breath-hold variations. While the majority of patients demonstrated acceptable target position variation within 5 mm, a subset exhibited substantial variability associated with reductions in target coverage.
A 5 mm threshold was used as a reference for clinically significant variation based on commonly reported planning target volume (PTV) margins in lung SBRT. However, margin strategies may vary across institutions depending on motion management and image guidance protocols. Therefore, the clinical impact of DIBH variability should be interpreted in the context of institution-specific margins, and variations exceeding local PTV margins may be of greater clinical significance.
It is important to note that the DIBH variations reported in this study reflect a combination of intra-fractional motion, inter-breath-hold variability, and residual setup uncertainties under routine clinical workflow conditions. Residual uncertainties may include image registration variability and target matching differences; therefore, the measured variation does not represent purely intrinsic breath-hold consistency. Unlike studies that evaluate breath-hold reproducibility without applying intermediate couch corrections, our approach incorporates repeated imaging and positional adjustments, which may influence the measured magnitude of variation. However, this methodology provides a more clinically representative assessment of target position consistency during actual treatment delivery.
In addition, beyond the initial pre-simulation coaching used to establish a reproducible DIBH level, no structured breathing validation or additional coaching was routinely implemented during treatment. Coaching was provided on an as-needed basis when patients experienced difficulty maintaining breath-hold. As such, the observed variability reflects standard clinical practice without enhanced training or verification protocols. The presence of large target position variations in a subset of patients suggests that additional coaching and validation strategies may improve breath-hold consistency and reduce intra-fraction variability.
An additional observation in this study was that DIBH variations were predominantly skewed toward negative values, particularly in the superior-inferior direction. This pattern may suggest that patients performed progressively shallower breath-holds during later imaging within a treatment fraction. One potential contributing factor is patient fatigue associated with repeated breath-hold attempts. Although DIBH was monitored using the RPM system, patients may compensate for reduced inspiratory depth through subtle body adjustments to satisfy surface monitoring criteria. For example, subtle body repositioning or back arching during shallower breath-holds may mimic deeper inspiration on surface tracking systems.
Patient #3 accounted for 8 of the 17 DIBH variations exceeding 5 mm, representing a major contributor to the overall variability. When this outlier was excluded, the proportion of DIBH variations exceeding 5 mm decreased from 11.71% (13/111) to 5.26% (5/95). This adjusted rate aligns closely with previously reported DIBH-related localization uncertainty of approximately 5 mm15. These findings suggest that, for most patients, target position variation remains clinically acceptable when appropriate implementation and monitoring are applied. This observation supports the influence of outlier patients on overall variability estimates and highlights the importance of individualized assessment.
The clinical implementation of DIBH is based on the premise that a consistent external respiratory signal is generally associated with reproducible internal target localization and anatomy. However, several sources of variability may affect this relationship. First, a single DIBH CBCT acquisition typically requires multiple breath-hold attempts, meaning that the reconstructed CBCT represents an average anatomical state across several DIBHs and may therefore contain inherent intra-CBCT variability. Second, despite similar external respiratory traces, anatomical differences may exist between separate DIBH CBCT acquisitions due to variations in breath-hold reproducibility. Third, additional anatomical variation may occur between DIBH imaging and actual treatment delivery despite comparable respiratory monitoring signals.
The current analysis focused on the second source of variability by evaluating differences between sequential DIBH CBCT acquisitions obtained within the same treatment fraction. The observed inter-CBCT differences may also provide indirect insight into anatomical variation that may occur between DIBH imaging and treatment delivery. However, intra-CBCT variability could not be directly evaluated with the available imaging tools, representing an important limitation of this study. Potential strategies to reduce this source of uncertainty include faster gantry rotation or reduced-/partial-arc CBCT acquisition techniques, where available.
Another limitation relates to the use of RPM-based respiratory monitoring as a surrogate for internal tumor position. Although RPM-guided DIBH is widely used clinically, external respiratory motion does not always perfectly correlate with internal tumor motion, particularly in thoracic malignancies. Consequently, similar external respiratory traces may still be associated with subtle internal anatomical differences. This limitation should be considered when interpreting the reproducibility of DIBH target localization observed in this study.
The worst-case scenario dose recalculations illustrated the potential clinical implications of persistent large DIBH variation. Worst-case scenario simulations assume sustained maximum displacement throughout treatment delivery, which may not be clinically realistic and therefore represent a conservative estimate of potential dosimetric impact. Due to the steep dose gradients characteristic of SBRT, target displacements exceeding standard PTV margins can result in significant reductions in GTV and PTV coverage. In the case of patient #13, the magnitude of DIBH variation exceeded the target dimension, resulting in a complete target miss under worst-case simulation. Although this represents an extreme scenario assuming sustained displacement throughout treatment, it highlights the theoretical risk associated with unrecognized or uncorrected DIBH variability. The dosimetric simulations performed in this study were limited to translational shifts and did not account for anatomical deformation or accumulated dose effects. Therefore, the simulated clinical impact may not fully represent actual delivered dose distributions and should be interpreted cautiously.
Simulated delivery analysis for patient #3 provided additional insight into the cumulative dosimetric impact of variable target position during DIBH across fractions. In this patient, the mean GTV V100% decreased from 99.91% in the planned scenario to 70.57% under simulated delivery. Similar reductions were observed for GTV V95% and PTV coverage metrics. These findings demonstrate that even when displacement fluctuates rather than persists at its maximum magnitude, cumulative underdosage may still occur.
Patient-specific factors likely contribute to variability in target positioning during DIBH. Patient #3 demonstrated the most frequent and largest DIBH variations across two separate treatment courses delivered approximately one year apart, suggesting persistent patient-specific limitations in breath-hold reproducibility. Potential contributing factors may include tumor location, pulmonary function, prior thoracic irradiation, age-related respiratory mechanics, and overall breath-hold tolerance. These findings further support the importance of individualized assessment during simulation to determine suitability for DIBH-based SBRT.
In addition, a trend toward reduced DIBH variation across treatment fractions was observed in patients who initially demonstrated larger displacements. This finding suggests a potential learning or adaptation effect, whereby repeated exposure and coaching may improve breath-hold consistency over time. Similar improvements in reproducibility with structured coaching and visual guidance have been reported in prior studies. These observations further support the potential benefit of incorporating targeted coaching and early-fraction monitoring into clinical workflows, particularly for patients demonstrating initial variability.
In this context, baseline pulmonary function and patient age may represent important clinical factors influencing DIBH performance and consistency. Pulmonary function tests (PFTs) provide an objective assessment of respiratory capacity and may help identify patients who are more likely to achieve stable and reproducible breath-holds. Similarly, age-related changes in respiratory mechanics and breath-hold tolerance may contribute to inter-patient variability. Although these parameters were not evaluated in the present study, future investigations incorporating PFT metrics and patient age may help establish clinically relevant predictors of DIBH performance and improve patient selection for DIBH-based SBRT.
From a clinical perspective, these findings support stratification of patients based on observed target position variation during DIBH. Patients demonstrating consistently low target position variation (<5 mm) may be considered favorable candidates for DIBH. Those exhibiting moderate but improvable variability may benefit from additional coaching and close intra-fraction monitoring. Conversely, patients with persistent large inter-breath-hold variation may be better managed using alternative motion management strategies, such as free-breathing with internal target volume (ITV) expansion. These findings highlight the importance of individualized motion management strategies based on patient-specific DIBH performance.
Strenghts and limitations
This study should be interpreted within the context of several methodological considerations. The sample size was limited and derived from a single institution, which may limit the generalizability of the findings. However, the cohort reflects routine clinical practice within a DIBH-based lung SBRT workflow and provides practical insight into real-world patterns of target position variation during DIBH.
Baseline pulmonary function test (PFT) data were not consistently available and therefore were not included in this analysis, although they may influence DIBH performance and reproducibility. Additionally, potential correlations between DIBH variability and patient-specific factors such as age or pulmonary function were not explored due to the limited sample size and data availability.
In addition, the analysis primarily relied on descriptive statistics, including mean values and standard deviations, to characterize DIBH variability. Repeated CBCT comparisons obtained from the same patient and treatment fraction were analyzed as independent observations, although these measurements may not be fully statistically independent. More advanced statistical approaches, such as separation of systematic and random errors or detailed patient-specific variability analysis, were not performed due to the limited sample size. Furthermore, no inferential statistical analysis (e.g., confidence intervals) was performed. Future studies with larger cohorts may allow for more comprehensive statistical evaluation.
The analysis relied on recorded couch shifts following CBCT-based alignment as a surrogate for inter-breath-hold target displacement. While this approach isolates DIBH variation after correction of setup error, it does not fully capture the complexity of tumor motion, including rotational errors, anatomical deformation, and baseline drift.
Consistent with this, the dosimetric analysis was based on rigid translational shifts applied to the treatment isocenter, reflecting the practical correction capability of the treatment system. Due to mechanical and workflow limitations, only translational couch corrections were applied, and these represent the closest achievable approximation to full six-degree-of-freedom (6DoF) adjustments in routine clinical practice. However, this approach does not account for rotational errors, anatomical deformation, or changes in internal anatomy (e.g., lung density or diaphragm position) between breath-holds. As such, the dosimetric impact of DIBH variability presented here should be interpreted as an approximation of the true delivered dose.
In addition, worst-case scenario simulations assumed sustained maximum displacement throughout treatment delivery, which may overestimate the clinical impact. To provide a more realistic representation, a simulated delivery approach incorporating randomly sampled DIBH variations was also performed. Furthermore, clinical outcome data such as local control or toxicity were not evaluated, and therefore direct correlation between DIBH variability and patient outcomes could not be established. Despite these limitations, the combined use of intra-fraction CBCT data and dosimetric modeling provides a clinically relevant assessment of DIBH performance and its potential impact on target coverage in lung SBRT.
Conclusion
Deep inspiration breath-hold is an effective motion management strategy for lung SBRT when consistent target positioning is maintained within clinically acceptable thresholds. In this study, the majority of patients demonstrated DIBH variation below 5 mm; however, a clinically meaningful subset exhibited substantial variability with measurable reductions in target coverage.
These findings highlight that DIBH consistency, as reflected by target position variation, is patient-dependent and cannot be assumed to be uniform across all individuals. Based on the observed variation patterns, patients may be tentatively categorized into three groups: (1) those with consistently reproducible DIBH (71.4%) suitable for standard implementation, (2) those requiring additional coaching and close intra-fraction monitoring (21.4%) to achieve acceptable reproducibility, and (3) those with persistent DIBH variability exceeding 5 mm (7.2%), for whom alternative motion management strategies such as free-breathing with ITV expansion may be more appropriate. This proposed classification is preliminary and hypothesis-generating, and requires validation in larger patient cohorts.
Careful patient selection during simulation, structured breath-hold coaching, and close intra-fraction monitoring are essential to ensure safe and effective DIBH-based lung SBRT delivery. When feasible, the use of internal surrogates, such as fiducial markers, may provide more reliable target localization than surface-based monitoring alone. Overall, this study provides preliminary clinically relevant insight that may help guide individualized motion management decision-making in lung SBRT.
Licence
© Author(s) 2026.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, and unrestricted adaptation and reuse, including for commercial purposes, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
References
-
Botticella A, Levy A, Auzac G, Chabert I, Berthold C, Le Pechoux C. Tumour motion management in lung cancer: a narrative review. Transl Lung Cancer Res. 2021;10(4):2011-7
-
Caillet V, Booth JT, Keall P. IGRT and motion management during lung SBRT delivery. Phys Med. 2017;44:113-22.
-
Mørkeset ST, Lervåg C, Lund J, Jensen C. Clinical experience of volumetric-modulated flattening filter free stereotactic body radiation therapy of lesions in the lung with deep inspiration breath-hold. J Appl Clin Med Phys. 2022;23(9):e13733.
-
Josipovic M, Persson GF, Bangsgaard JP, Specht L, Aznar MC. Deep inspiration breath-hold radiotherapy for lung cancer: impact on image quality and registration uncertainty in cone beam CT image guidance. Br J Radiol. 2016;89(1068):20160544.
-
Naumann P, Batista V, Farnia B, et al. Feasibility of optical surface-guidance for position verification and monitoring of stereotactic body radiotherapy in deep-inspiration breath-hold. Front Oncol. 2020;10:573279.
-
Lawler G. A review of surface guidance in extracranial stereotactic body radiotherapy (SBRT/SABR) for set-up and intra-fraction motion management. Tech Innov Patient Support Radiat Oncol. 2022;21:23-6.
-
Nguyen D, Reinoso R, Farah J, et al. Reproducibility of surface-based deep inspiration breath-hold technique for lung stereotactic body radiotherapy on a closed-bore gantry linac. Phys Imaging Radiat Oncol. 2023;26:100448.
-
Prado A, Zucca D, De la Casa MÁ, et al. Intrafraction target shift comparison using two breath-hold systems in lung stereotactic body radiotherapy. Phys Imaging Radiat Oncol. 2022;22:57-62.
-
Shah C, Grills IS, Kestin LL, et al. Intrafraction variation of mean tumor position during image-guided hypofractionated stereotactic body radiotherapy for lung cancer. Int J Radiat Oncol Biol Phys. 2012;82(5):1636-41.
-
Scherman Rydhög J, Riisgaard de Blanck S, Josipovic M, et al. Target position uncertainty during visually guided deep-inspiration breath-hold radiotherapy in locally advanced lung cancer. Radiother Oncol. 2017;123(1):78-84.
-
Aznar MC, Carrasco de Fez P, Corradini S, et al. ESTRO-ACROP guideline: recommendations on implementation of breath-hold techniques in radiotherapy. Radiother Oncol. 2023;185:109734.
-
Josipovic M, Aznar MC, Thomsen JB, et al. Deep inspiration breath hold in locally advanced lung cancer radiotherapy: validation of intrafractional geometric uncertainties in the inhale trial. Br J Radiol. 2019;92(1104):20190569.
-
Boda-Heggemann J, Knopf AC, Simeonova-Chergou A, et al. Deep inspiration breath hold–based radiation therapy: a clinical review. Int J Radiat Oncol Biol Phys. 2016;94(3):478-92.
-
Peng Y, Vedam S, Chang JY, et al. Implementation of feedback-guided voluntary breath-hold gating for cone beam CT-based stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys. 2011;80(3):909-17.
-
Keall PJ, Mageras GS, Balter JM, et al. The management of respiratory motion in radiation oncology: report of AAPM Task Group 76. Med Phys. 2006;33(10):3874-900.