







Barriers and Facilitators of Oral Nutritional Supplement Adherence in Cancer: A Systematic Review
Abstract
Background: Cancer-related malnutrition is highly prevalent yet frequently underrecognised in oncology practice and is associated with adverse outcomes, including reduced treatment tolerance, impaired quality of life, and decreased survival. Oral nutritional supplements (ONS) are recommended as first-line nutritional support for patients unable to meet their energy and protein requirements through diet alone. However, adherence to ONS is often suboptimal, limiting its clinical effectiveness.
Aim: This systematic review aimed to identify and synthesise the barriers and facilitators influencing adherence to oral nutritional supplements (ONS) among adult cancer patients, with particular attention to patient-centred experiences and contextual determinants.
Methodology: A systematic search of PubMed/MEDLINE, CINAHL, Scopus, Web of Science, and Embase was conducted for studies published between 1 January 2021 and 4 January 2026. Qualitative, quantitative, and mixed-methods studies examining barriers and/or facilitators to ONS adherence in adult cancer populations were eligible. Study selection, data extraction, and methodological appraisal were performed independently by two reviewers in accordance with PRISMA 2020.
Results: Twelve studies published between 2021 and 2025 were included. Barriers to ONS adherence clustered within four interacting domains: symptom- and treatment-related factors (e.g., gastrointestinal intolerance and taste alterations), patient-related cognitive and behavioural factors (e.g., misconceptions, low perceived benefit, reduced self-efficacy), product-related attributes (e.g., palatability and volume), and healthcare system and financial-contextual determinants (e.g., limited follow-up and reimbursement barriers). Facilitators included proactive symptom management, personalised and preference-based ONS regimens, structured education and behavioural support, multidisciplinary follow-up, caregiver involvement, and supportive reimbursement mechanisms.
Conclusion: ONS adherence in adult cancer patients is shaped by a complex interplay of clinical, behavioural, product-related, and system-level determinants. Suboptimal adherence may reflect treatment-related burden and implementation challenges rather than patient unwillingness alone. Effective strategies should integrate symptom-responsive care, individualised nutritional counselling, structured follow-up, and system-level support mechanisms within coordinated oncology pathways. Future research should prioritise standardised adherence measurement and implementation-focused intervention models to enhance the real-world impact of nutritional support in cancer care.
Keywords: Adherence; Barriers; Cancer; Facilitators; Oral nutritional supplements; Systematic review
Introduction
Malnutrition in patients with cancer is a frequent and clinically significant problem due to the disease process and the treatment modalities. Prevalence of malnutrition is reported to vary according to type of cancer, its stage, and the used diagnostic criteria from 24% to 55%1. Consequences of cancer related malnutrition are reduced tolerance to treatment, increased risk of complications, extended length of hospital stay, diminished quality of life and possibly impaired survival2,3. Thus, oral nutritional supplements (ONSs) are first‐line nutritional support in prevention and treatment of malnutrition in patients with cancer who are unable to maintain adequate energy and nutrient intake by ordinary diet2. ONSs are designed to deliver energy, protein, and micronutrients in a small volume and easy-to-consume format. Oral nutritional supplements (ONS) are effective interventions for improving nutritional status, maintaining treatment intensity and reducing complications if administered adequately4. However, the clinical effectiveness of ONS is influenced by not only its nutrient composition, but also the adherence of the patients to the recommended regimen. To date, the adherence to ONS among cancer patients reported in literature is poor and presents high variability according to studies. Adherence rates reported in the literature can vary between 6 and more than 90%, indicating that the behavior of adherence is multi- dimensional and complex5. In addition, not following the recommend- ations of ONS will result in losing the expected benefits of vital energy and nutrition; thus leading to insufficient nutrient ingestion, reduced treatment efficacy, raised cost of healthcare and product wastage6.
Recently published results of studies indicate that determinants of ONS adherence cannot be fully explained by personal will or prescription of the product, but are affected by a range of factors related to the patient, the product, the healthcare system, and the social context. The most common reasons for non-compliance are gastrointestinal intolerance, dissatisfaction with its organoleptic characteristics, such as taste and smell, burden of cancer or treatment-related symptoms, and misinformation related to ONS content (e.g. that sugar feeds tumour)7,8,9. On the other hand, personalized nutritional advice, frequent follow-up, support from dietitians and nurses, perceived benefit, and flexible application that accommodates the patients’ preferences are considered the facilitators for compliance to ONS5,10.
Qualitative studies published in the last 5 years indicate that patients’ experiences and health beliefs concerning ONS are critical for adherence. The results of these two systematic reviews suggest that a large proportion of cancer patients consider ONS as ‘a medical necessity to get through’ rather than a source of nutrition and this might be connected to medicalisation of eating behaviour11,12.
This opinion could adversely impact motivation for long-term and regular use even if the patients realize the advantageous features of ONS. Moreover, a lack of education, low degree of patient participation in the decision- making process and not enough support for self-efficacy are some of the significant elements which undermined the persistence of high level of adherence13.
While the present systematic and scoping reviews on adherence to ONS; The majority of the studies in most cases are conducted with mixed patient populations, specific types of cancer, or focuses on clinical outcomes, and therefore do not adequately consider experiences of patient with a holistic perspective5,8. In addition, the large variation in the conceptualization and assessment of adherence complicate the comparability and clinical translation of results14. This scenario necessitates an up-to-date and focused synthesis. This systematic review aims to be the first to explore and thematically frame barriers and facilitators to oral nutritional supplement adherence in adult cancer patients, as described in studies from the last 5 years. Integrating qualitative, quantitative, and mixed-method studies, the intent is to offer a patient-centric and comprehensive understanding of ONS adherence. The results of this study are expected to inform clinical practice, help to develop specific interventions, and provide theoretical foundation for further studies developing measurement tools.
The aim of the study was to describe the barriers for and facilitators of oral nutritional supplement (ONS) adherence among adult patients with cancer using a narrative synthesis. Results: The review combines qualitative and quantitative findings of studies and mixed-method study designs published in the last five years, with the purpose of answering a patient-related, single product, and disease specific question, from patient, product, healthcare system and social context perspective concerning factors influencing adherence to ONS. It is anticipated that the findings will support advancement in clinical practice, inform design of targeted interventions, and provide a theoretical basis for future instrument development and intervention research.
Methodology
Research Questions
This systematic review seeks to answer the following research questions:
- What are the main barriers and facilitators to adherence to oral nutritional support (ONS) in adult cancer patients?
Secondary/Sub-research questions - How does the symptom burden associated with cancer treatment (especially gastrointestinal symptoms and sensory changes) affect adherence to ONS?
- How do patient-related cognitive and behavioral factors (misconceptions, perceived benefit, self-efficacy) play a role in maintaining ONS use?
- How do ONS product characteristics (taste, texture, volume, formulation, and duration of use) shape adherence behavior?
- How do health system-related factors (frequency of follow-up, continuity of care, multidisciplinary approach, post-discharge support) affect adherence to ONS?
- How do financial and social contextual factors (reimbursement, financial burden, family/caregiver support) affect long-term adherence to ONS?
- To what extent are interventions such as structured monitoring, individualized nutritional counseling, and caregiver involvement reported to support or enhance adherence to ONS?
Study Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines¹⁵. The aim of the review was to synthesise the barriers and facilitators influencing adherence to oral nutritional supplements (ONS) among adult cancer patients. Qualitative, quantitative, and mixed-methods studies were included to provide a comprehensive synthesis of factors affecting ONS adherence.
Predefined eligibility criteria, structured search strategies, and independent study selection and data extraction procedures were applied to ensure methodological transparency and rigour.
Inclusion and Exclusion Criteria
Inclusion criteria:
- Studies involving cancer patients aged ≥18 years
- Studies examining oral nutritional supplement (ONS) adherence
- Studies reporting barriers and/or facilitators affecting ONS adherence
- Qualitative, quantitative, or mixed-methods studies
- Studies published in peer-reviewed journals
- Studies published in English between January 1, 2021, and January 4, 2026
Exclusion criteria:
- Studies involving pediatric populations
- Studies focusing on enteral or parenteral nutrition
- Studies evaluating only the clinical efficacy of ONS without adherence-related outcomes
- Reviews (systematic, narrative, or scoping), editorials, commentaries, letters, theses, and conference proceedings
- Publications with unavailable full text
Literature Search Strategy
A systematic literature search was conducted in the following electronic databases: PubMed/MEDLINE, CINAHL, Scopus, Web of Science, and Embase. The search covered studies published between January 1, 2021, and January 4, 2026, with no restrictions regarding cancer type, stage, or treatment modality. The final search was conducted on January 4, 2026. Search terms were developed based on the review objectives and combined controlled vocabulary (e.g., MeSH terms in PubMed) and free-text keywords. The core search strategy included terms related to oral nutritional supplements (“oral nutritional supplements,” ONS, “sip feed”), adherence (“adherence,” compliance, uptake, persistence), cancer (“cancer,” oncology, neoplasm), and determinants (“barriers,” facilitators, experiences, perceptions), combined using Boolean operators (AND/OR). The search strategy was adapted for each database using appropriate controlled vocabulary and syntax.
The literature search and study screening processes were conducted independently by two researchers. Reference lists of included studies were also manually screened to identify additional relevant publications.
Study Selection Process
All records identified through the database search were imported into reference management software, and duplicate records were removed. Study selection was conducted in two stages. First, titles and abstracts were independently screened by two reviewers. Second, the full texts of potentially eligible studies were assessed for inclusion. Any disagreements between the reviewers were resolved through discussion until consensus was reached.
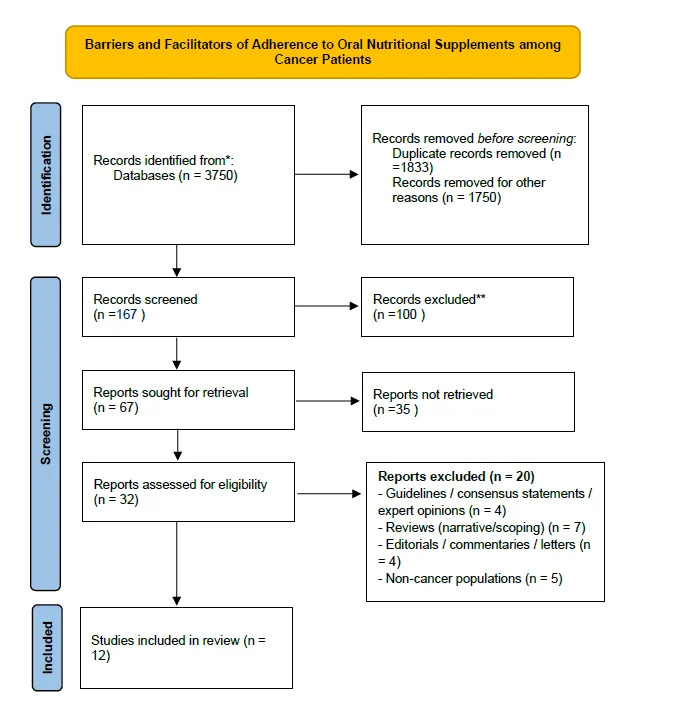
The study selection process is illustrated using the PRISMA 2020 flow diagram (Figure 1).
Figure 1. PRISMA 2020 flow diagram
Data Extraction
Data extraction was performed independently by two researchers, and discrepancies were resolved through discussion. The following information was obtained from the included studies using a standard data extraction form:
- Author(s) and year of publication
- Country
- Study design
- Sample characteristics (cancer type, number of patients)
- Type of ONS and context of use
- Definition and evaluation method of ONS adherence
- Barriers affecting ONS adherence
- Facilitators affecting ONS adherence
- Theoretical framework used (if any)
Quality Assessment
The methodological quality of the included studies was considered during the interpretation of the findings. Due to the heterogeneity of study designs and outcomes across the included studies, a formal critical appraisal using standardized appraisal tools was not conducted.
Data Synthesis
The findings were synthesised using narrative and thematic synthesis approaches. Barriers and facilitators influencing adherence to oral nutritional supplements (ONS) were identified and coded based on recurring patterns and organised into four overarching thematic domains: patient-related factors, product (ONS)-related factors, health system-related factors, and social and environmental factors. Qualitative and quantitative findings were integrated within this thematic framework to provide a holistic synthesis of factors influencing adherence behaviour.
Ethical Considerations
Since this study is a secondary analysis of published research, it does not require ethical committee approval.
Results
A total of 12 studies published between 2021 and 2025 were included in the final synthesis (Table 1)5,8,9,16,17,18,19,20,21,22,23,24. The included evidence comprised meta-analyses, systematic reviews, mixed-methods systematic reviews, a systematic mixed-studies review, a qualitative descriptive study, an evidence summary, a narrative review, and one mixed-methods study protocol. Studies were conducted across multinational and national settings, including Europe, Canada, Australia, Asia, China, Greece, Ireland, and Thailand, reflecting variability in healthcare systems and cancer care contexts.
Table 1. Characteristics of Included Studies on ONS Adherence Determinants and Supporting Evidence in Adult Cancer Patients (2021–2025)
| Study (Author/ | Country | Study Design | Cancer Type / Setting | Sample Size (n) | Barriers | Facilitators |
|---|---|---|---|---|---|---|
| Year) | ||||||
| Raso et al., 2025 | Multinational (Europe, Canada, Australia, Asia) | Meta-nalysis | Gastrointestinal cancers / preoperative prehabilitation programs | 40 studies, n = 1619 | Longer intervention duration; multimodal programmes (lower adherence vs unimodal); common barriers included logistics, exercise intensity, time constraints, and tolerance to nutritional supplements; low adherence to psychological support component | Higher adherence in unimodal programmes; higher adherence to nutrition and exercise components; shorter intervention duration; potential enablers include structured behavioural strategies and digital tools. |
| Liu et al., 2025 | China | Qualitative descriptive study (Social Cognitive Theory–based, semi-structured interviews) | Mixed cancer types / tertiary cancer hospital, inpatient setting | n = 14 | Misconceptions about ONS, intake-related GI symptoms and sensory discomfort (sweetness, viscosity, bloating, diarrhea), low self-efficacy, misinformation from non-professional sources, product incompatibility (portion size, taste, solubility), financial burden and financial burden and limited reimbursement/coverage, lack of continuity of care after discharge | Accurate understanding of ONS benefits, higher self-efficacy, self-monitoring and reminder strategies, adaptive coping behaviors (mixing, dose adjustment), structured follow-up by healthcare professionals, family support, peer support, practical use of digital or non-digital reminder tools |
| Lin et al., 2025 | China-dominant (13 China + 1 UK) | Mixed-methods systematic review | GI neoplasm patients (≥18y) | 14 studies; total n=1,874 | Adverse reactions + treatment side effects; low perceived benefit; palatability/texture issues; inadequate support | Symptom management; education improving perceived benefit; follow-up/monitoring; individualized adjustments |
| Wang et al., 2025 | China | Systematic literature search in Chinese and English databases | Postoperative gastric cancer / home nutritional management | 15 included evidence documents | Lack of systematic practical guidance for home nutrition management; limited self-management skills and family support | Best evidence recommendations: nutritional monitoring/assessment, multidisciplinary teamwork, symptom management, post-discharge follow-up, and digital/“Internet+” home nutrition support |
| Liljeberg et al., 2025 | Multinational | Systematic mixed-studies review | Adults with malnutrition (including malignancy/cancer populations) | 171 studies | Poor taste, GI intolerance, high cost, long treatment duration, inadequate healthcare routines | Good product tolerance, small-volume/high-density ONS, reimbursement, family support, well-functioning healthcare systems |
| Lidoriki et al., 2024 | Greece | Systematic review | Gastrointestinal cancer patients undergoing surgery and/or chemotherapy | 11 studies (included), n = 2.518 | Gastrointestinal symptoms (diarrhea, bloating, early satiety), nausea and vomiting, taste alterations, texture/flavor dislike, large volume of ONS, appetite loss, psychosocial factors (anxiety, depression), low motivation | Regular monitoring, personalized nutritional counseling, early identification and management of side effects, patient education, caregiver support, tailored ONS regimens |
| Baguley et al., 2024 | Australia | Systematic review | Older cancer patients (≥65y) / nutrition interventions | 11 studies (9 RCTs) | Intervention-focused (indirect relevance to ONS adherence; highlights research gaps) | Highlights need for consistent reporting of dietary prescription and adherence; supports importance of structured nutrition counselling and ONS where indicated |
| Sa-nguansai et al., 2024 | Thailand | Systematic review & meta-analysis of RCTs | Adult cancer patients receiving chemotherapy | 10 RCTs; n=1,101 | Focuses on clinical effectiveness of ONS | ONS may improve weight change (esp. elderly/female/low baseline weight/non-Asian) and improves QoL outcomes (global QoL, fatigue) |
| Ghias et al., 2023 | Ireland | Review | Cancer patients receiving chemotherapy/radiotherapy (treatment-induced dysgeusia) | Review article; no participant sample) | Treatment-induced dysgeusia and reduced sensory perception leading to decreased desire to eat, reduced food intake, and reduced consumption of oral nutritional supplements, contributing to malnutrition/pre-cachexia | Facilitators (indirect): improving ONS palatability/acceptability, individualized nutrition interventions, addressing taste alterations to enhance ONS uptake |
| Wang et al., 2022 | China | Mixed-methods (literature review + in-depth interviews + focus groups; DCE attribute development) | Gastric cancer (post-gastrectomy, postoperative period) | n = 15 (interviews) + n = 19 (focus groups) | Adverse gastrointestinal reactions (e.g., bloating, diarrhea), poor taste/flavor, cost and lack of reimbursement, inconvenience of preparation, uncertainty about benefits. | Professional guidance (dietitian/physician/nurse), one-to-one education, regular follow-up (method/frequency), psychological support, clear information on benefits, variety of flavors |
| Wang et al., 2023 | Multinational | Systematic review | Various adult cancers / hospital & community settings | 18 studies total, n = 1,267 | GI intolerances and disliked tastes (most frequent barriers); other reported barriers included large volume and treatment-related symptoms. | ONS management strategy (most crucial facilitator), regular monitoring, professional guidance, education, symptom management. |
| Wan et al., 2021 | China | Mixed-methods study protocol (12-week longitudinal + qualitative; explanatory sequential design) | Gastric cancer patients after gastrectomy | n = 135 | Results not yet available (protocol) | Planned adherence monitoring/support: weekly ONS diary and WeChat-based follow-up; integration of quantitative and qualitative findings to inform adherence improvement strategies |
The majority of studies focused on adult cancer populations, particularly gastrointestinal cancers in preoperative, postoperative, and chemotherapy settings. Some studies provided indirect or contextual evidence on ONS adherence through broader nutrition intervention research or symptom-related mechanisms such as dysgeusia⁸˒¹⁶˒¹⁹. One mixed-methods protocol aimed to evaluate adherence trajectories in postoperative gastric cancer patients; however, results were not yet available⁹.
Study Characteristics and Sample Sizes
As summarised in Table 1, the included studies demonstrated considerable heterogeneity in design and sample characteristics. A systematic review including 11 studies (n = 2,518)⁸ examined patients undergoing surgery and/or chemotherapy. A mixed-methods systematic review synthesised evidence from 14 studies (n = 1,874)¹⁶, focusing on determinants of adherence in gastrointestinal neoplasms. A meta-analysis of prehabilitation programmes in gastrointestinal cancer included 40 studies (n = 1,619)²¹ and examined adherence differences between unimodal and multimodal interventions.
Table 1 further shows that a systematic mixed-studies review incorporated 171 studies¹¹ involving malnourished populations, including cancer subgroups. Primary research also included a mixed-methods study involving postoperative gastric cancer patients (n = 15 interviews; n = 19 focus groups)¹⁷ and a qualitative descriptive study based on Social Cognitive Theory (n = 14)²².
Additionally, as presented in Table 1, a multinational systematic review synthesised 18 studies (n = 1,267)⁵ examining barriers and facilitators of ONS adherence. One mixed-methods protocol proposed a 12-week adherence evaluation (planned n = 135)⁹. An evidence summary including 15 documents provided recommendations for home nutritional management²³.
Barriers to Adherence to Oral Nutritional Supplements
As shown in Table 1, barriers to ONS adherence were consistently reported and can be grouped into four main domains: symptom- and treatment-related factors, patient-related factors, product-related factors, and system-level determinants5,8,17,21,22,24.
Symptom- and treatment-related barriers
Table 1 indicates that gastrointestinal symptoms such as diarrhea, bloating, early satiety, nausea, vomiting, and appetite loss were frequently reported barriers, particularly in gastrointestinal cancer populations. Treatment-related side effects and adverse reactions also negatively affected adherence. Taste alterations, including dysgeusia, were identified as key mechanisms reducing desire to consume ONS and overall intake8,16,19.
Patient-related barriers
As detailed in Table 1, patient-level barriers included misconceptions about ONS, uncertainty about its benefits, and low self-efficacy. Misinformation from non-professional sources and negative beliefs further reduced adherence19,22.
Product-related barriers
Table 1 further demonstrates that sensory characteristics such as poor taste, unpleasant texture, and large volume requirements were major barriers. Additional issues included gastrointestinal intolerance, product incompatibility, and prolonged treatment duration17,22,24.
System-level barriers
As presented in Table 1, financial burden, limited reimbursement, lack of structured guidance, and insufficient continuity of care after discharge were commonly reported. In complex multimodal interventions, longer duration and programme burden were associated with lower adherence17,21,22,23.
Facilitators of ONS Adherence
Consistent with the evidence summarised in Table 1, facilitators of adherence were consistently associated with structured clinical support, symptom management, and behavioural strategies, with additional system-level enabling factors5,8,16,17,21,22,23,24.
Professional support and monitoring
Table 1 highlights that regular follow-up, professional guidance, and structured monitoring were among the most important facilitators. Multidisciplinary approaches, nutritional assessment, and continuous post-discharge support improved adherence. Digital tools and follow-up systems were also identified as potential enablers9,22,23.
Behavioural and educational facilitators
As shown in Table 1, improved understanding of ONS benefits, increased self-efficacy, and self-management strategies (e.g., reminders, self-monitoring, adaptive use) supported adherence. Education and structured behavioural strategies were consistently highlighted16,22.
Product and system-related facilitators
Table 1 also demonstrates that better product tolerance, including small-volume and high-density formulations, enhanced adherence. Reimbursement mechanisms, family and peer support, and well-functioning healthcare systems also facilitated sustained use20,24.
Summary of Main Themes
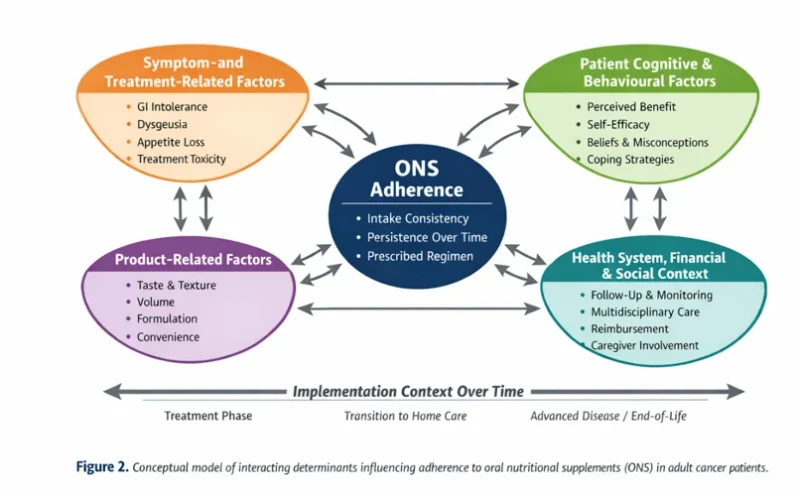
Overall, as synthesised from Table 1, four overarching domains emerged as determinants of ONS adherence in adult cancer patients: (1) symptom burden and treatment-related effects, (2) patient cognitive and behavioural factors, (3) product-related characteristics, and (4) healthcare system and support mechanisms.
These domains interact dynamically and collectively shape adherence behaviour across different stages of cancer care. ONS adherence is therefore best understood as a multidimensional and context-dependent outcome influenced by clinical, behavioural, product-related, and system-level factors rather than a solely patient-driven behaviour (Table 2).
Table 2. Thematic Summary of Barriers and Facilitators Influencing ONS Adherence in Adult Cancer Patients
| Domain | Barriers to Adherence | Facilitators of Adherence |
|---|---|---|
| Symptom- and Treatment-Related Factors | • Gastrointestinal intolerance (nausea, vomiting, diarrhea, bloating, early satiety) | • Proactive symptom management |
| • Appetite loss | • Early identification and management of adverse effects | |
| • Treatment-induced dysgeusia and altered sensory alterations | • Adjustment of timing and intake strategies | |
| • Overall symptom burden reducing tolerance and acceptability | • Integration of nutritional care with oncology symptom control | |
| Patient Cognitive and Behavioural Factors | • Misconceptions and negative beliefs about ONS | • Individualised education focused on practical use |
| • Low perceived benefit | • Enhancement of perceived benefit | |
| • Reduced motivation | • Strengthening self-efficacy | |
| • Low self-efficacy | • Self-monitoring and reminder strategies | |
| • Influence of non-professional information sources | • Adaptive coping behaviours (e.g., mixing, dose adjustment) | |
| Product-Related Factors | • Poor taste and texture | • Small-volume/high-density formulations |
| • Excessive sweetness | • Flavour variety | |
| • Large required volume | • Personalised or preference-based regimens | |
| • Preparation burden | • Flexible dosing approaches | |
| • Long duration of prescribed use | • Improved product tolerability | |
| Health System, Financial, and Social Context Factors | • Limited follow-up and poor continuity of care post-discharge | • Multidisciplinary follow-up |
| • Lack of structured monitoring | • Structured monitoring systems (e.g., diaries, digital tools) | |
| • Financial burden and inadequate reimbursement | • Reimbursement mechanisms | |
| • Programme complexity in multimodal interventions | • Caregiver involvement and family support | |
| • Well-functioning healthcare routines |
Discussion
This review highlights that adherence to oral nutritional supplements (ONS) in adult cancer populations should be conceptualised as a multidimensional behavioural and clinical outcome rather than a simple measure of patient “compliance.” Although ONS is commonly prescribed as a first-line nutritional strategy, adherence remains difficult to achieve in routine oncology care because it is shaped by interacting symptom burden, product acceptability, psychosocial processes, and the organisation of supportive care services2,3,6,8,16,24. Accordingly, the present synthesis supports a shift from viewing suboptimal adherence as a patient deficit to understanding it as an indicator of the fit between nutritional therapy and patients’ lived treatment experiences, as well as the quality of continuity and implementation of nutrition care5,23.
Barriers to ONS adherence: interpretation and underlying mechanisms
A central insight from the included evidence is that the most salient barriers to ONS adherence often originate from cancer- and treatment-related physiological changes. In this context, reduced intake should not automatically be interpreted as unwillingness or poor motivation. Instead, adherence behaviours may reflect a rational adaptation to symptom burden and treatment toxicity. Gastrointestinal intolerance, including nausea, early satiety, diarrhoea, bloating, vomiting, and appetite loss, can directly constrain the amount of ONS that can be consumed and can reduce motivation by reinforcing negative experiences related to eating2,6,8,16,17. These findings imply that adherence interventions focused solely on education are unlikely to be effective if symptoms are not adequately controlled.
Alterations in taste sensation and dysgeusia represent major barriers to ONS adherence. Treatment-related dysgeusia interferes with sensory pleasure and food perception, which may contribute to diminished desire to eat and lower supplement intake over time7,19. Sensory symptoms may therefore operate as both physiological and behavioural barriers, increasing aversion and “sensory fatigue,” particularly when ONS is prescribed for prolonged periods7,19. These observations further support the notion that adherence and symptom management are inextricably linked: if dysgeusia and other sensory changes are not addressed, expectations for sustained adherence may be unrealistic, especially during chemo- and radiotherapy8,19.
Barriers also appear to be compounded by cognitive and motivational processes. Misconceptions about ONS and doubts regarding its benefits may arise not only from limited education, but also from patients’ interpretations of ongoing symptoms and the absence of perceived short-term improvement. When patients experience persistent distress despite supplementation, they may conclude that little benefit is achievable and reduce intake. This underscores the need for education that aligns with realistic expectations, addresses short-term symptom-related goals, and provides practical strategies rather than focusing exclusively on long-term nutritional outcomes3,16,17,22. Similarly, low self-efficacy may emerge after repeated unsuccessful attempts to tolerate ONS; therefore, efforts to enhance confidence should be delivered as symptom-responsive counselling combined with actionable coping plans rather than as generic motivational messages22.
At the system level, discontinuity of care-particularly during the transition from hospital to home-emerges as a structural determinant of nonadherence. ONS prescriptions often require substantial self-management at a time when patients may be fatigued, psychologically distressed, and managing complex medication regimens2,5,23. Limited follow-up and inconsistent practical education suggest that barriers may reflect deficiencies in service delivery and implementation fidelity rather than problems attributable solely to the patient or the product2,4. In this regard, difficulties with adherence may indicate that nutritional therapy is being prescribed without sufficient infrastructure to support its execution in real-world conditions.
Financial strain further intensifies these challenges and raises equity concerns. When ONS is not funded or coverage is partial, sustained use becomes contingent on patients’ financial resources, introducing socioeconomic disparities in access to supportive care17,24. This is consistent with broader evidence on access barriers within oncology supportive care and patient assistance pathways25. From both ethical and implementation perspectives, adherence strategies that overlook affordability may preferentially benefit those with greater resources and may have limited scalability across healthcare settings24,25.
Finally, intervention complexity itself may create adherence burden. Evidence from prehabilitation research indicates that multimodal programmes can reduce adherence relative to unimodal approaches, particularly when patients have limited capacity to engage with multiple components during intensive treatment periods12,21. Accordingly, adherence should be conceptualised as a balance between clinical ambition and behavioural feasibility, and intervention designs should account for treatment burden and competing demands12,21.
Facilitators of ONS Adherence: Actionable Enablers and Implementation Considerations
Facilitators can be conceptualised as processes that enhance the alignment between ONS therapy and the patient’s clinical and social context. Professional support, particularly within multidisciplinary teams that include dietitians and nursing input, appears effective not only because it provides information but also because it enables iterative problem-solving and timely adjustment of nutritional plans2,3,5,8,16. ONS adherence is likely to benefit from structured follow-up, enabling clinicians to monitor tolerance, adjust prescriptions as needed, and respond to evolving symptom trajectories2,3,5,8,16. This underscores the importance of conceptualising ONS as a dynamic therapeutic intervention rather than a static prescription2,3.
Regular monitoring and structured follow-up may also strengthen continuity and accountability, but these processes should be framed as supportive rather than surveillance-oriented, normalising challenges and offering practical solutions. Digital approaches (e.g., app-based monitoring or messaging platforms such as WeChat) may enhance continuity of care in resource-limited contexts and mitigate post-discharge attrition, thereby facilitating implementation of guideline-recommended nutritional pathways4,9,23.
Product-based enablers further indicate that adherence improves when ONS regimens are personalised. Flexibility and preference-based approaches may enhance autonomy, reduce aversion, and improve acceptability, particularly among patients experiencing gastrointestinal intolerance or taste changes8,16,17,24. Practical adjustments-such as offering flavour variety, selecting small-volume/high-energy formulations, and using flexible dosing schedules-may reduce the perceived burden of intake and support sustained use24.
Education remains relevant but functions as a facilitator when it is structured, standardised, and linked to pragmatic coping strategies. Patients are likely to derive greatest benefit from education that emphasises actionable guidance (e.g., timing of intake relative to symptoms or medications, strategies to improve palatability, dose titration, and integration into daily routines) rather than abstract nutritional concepts3,19,25. In this way, education can strengthen perceived benefit and self-efficacy by ensuring that patients have a feasible “plan B” when barriers arise22.
Caregiver involvement also appears to facilitate adherence, particularly in home-care contexts where cancer-related fatigue, functional limitations, and psychological distress may hinder sustained self-management22,24. Caregivers may support habit formation, preparation, and emotional coping; however, caregiver availability and capacity vary. Interventions should therefore assess caregiver resources and provide parallel support, rather than shifting the burden of care from healthcare systems to families23,24.
At the systems level, reimbursement and supportive service structures function as facilitators by stabilising access and reducing financial barriers. Nutritional support is more likely to be effective when delivered through structured pathways that include discharge planning, follow-up routines, and equitable coverage mechanisms4,23,24. These system-level processes may be as influential as patient-facing interventions in determining sustained adherence.
Importantly, symptom control and pharmacological management may be integral to successful adherence support, yet were inconsistently described across the included studies. Future implementation research should therefore evaluate integrated supportive care models that coordinate ONS prescriptions with symptom-directed pharmacotherapies (e.g., antiemetics, antidiarrhoeals, analgesia, appetite stimulants when appropriate) and structured nutritional counselling. Such integration may improve feasibility of intake and clarify the pathways through which symptom management enables sustained adherence.
In summary, this evidence indicates that improving ONS adherence is more a matter of delivering nutritional care than merely prescribing supplements. Effective strategies should combine symptom-responsive management, preference-informed product selection, structured follow-up, and explicit attention to affordability within coordinated oncology care pathways in line with ESPEN recommendations2. Future research should prioritise standardised measurement of adherence, theory-informed intervention design, and evaluation of scalable follow-up models, alongside economic and equity-focused analyses to ensure that adherence-support strategies are feasible across diverse healthcare systems25.
While several included studies have also contributed to previous reviews on nutritional support in oncology, the present review provides an updated synthesis covering 2021–2025 and focuses specifically on adherence to ONS in adult cancer populations. Its added value lies not in generating new primary data, but in integrating qualitative, quantitative, and mixed-methods evidence within a unified thematic framework. By organising determinants into interacting symptom-, patient-, product-, and system-level domains, this review advances a patient-centred and implementation-oriented understanding of ONS adherence, with practical relevance for clinical care and future intervention development.
Ethical and Clinical Considerations in Advanced Disease and End-Of-Life Transitions
The use of oral nutritional supplements (ONS) in advanced disease and during transitions to end-of-life care involves important ethical and clinical considerations. Although nutritional support may enhance comfort, function, and treatment tolerance in earlier stages, its goals and expected benefits should be re-evaluated when disease progression is irreversible and symptom burden is substantial. In such contexts, adherence should not be framed as a moral obligation; rather, decisions regarding continuation or discontinuation of ONS should align with patient values, proportionality of benefit, and the practical feasibility of intake under refractory symptoms.
Effective decision-making requires shared discussions that integrate symptom burden, expected clinical benefit, and patient preferences. Coordination of ONS prescriptions with symptom-directed pharmacotherapy (e.g., antiemetics, appetite stimulants, analgesics) is essential to ensure that nutritional recommendations remain clinically appropriate and tolerable. Without adequate symptom control, continued ONS use may increase distress rather than contribute to wellbeing.
When the primary goals of care shift toward comfort, nutritional interventions-including ONS-should be considered within broader goals-of-care discussions. In these circumstances, avoiding non-beneficial interventions and respecting the patient’s understanding of quality of life and a “good death” become central ethical principles guiding clinical practice.
Strengths and Limitations
A key strength of this review is the inclusion of methodologically diverse evidence (qualitative, quantitative, mixed-methods, and evidence syntheses) across multiple international healthcare contexts, enabling a comprehensive understanding of determinants influencing adherence to oral nutritional supplements (ONS) in adult cancer populations. Thematic synthesis allowed integration of findings despite variability in study designs and outcome reporting.
Several limitations should be acknowledged. First, many primary studies relied on self-reported adherence measures, which are susceptible to recall and social desirability bias and may overestimate true adherence. Second, substantial heterogeneity in adherence definitions, measurement approaches, and reporting thresholds limited direct comparability and precluded meta-analysis. Third, the evidence base was disproportionately weighted toward gastrointestinal cancer populations and certain geographic regions, potentially limiting generalisability to other cancer types and healthcare systems. Finally, overlap of primary studies across evidence syntheses may have influenced the relative emphasis of specific barriers and facilitators.
Because symptom burden emerged as a central determinant of adherence, the limited and inconsistent reporting of integrated pharmacological and symptom-management pathways alongside ONS use represents an important evidence gap. Few studies explicitly examined how appetite stimulants, antiemetics, or other symptom-directed pharmacotherapies were coordinated with nutritional interventions, highlighting the need for implementation-focused research addressing integrated supportive care models.
Conclusion
This systematic review demonstrates that adherence to oral nutritional supplements (ONS) in adult cancer patients is a complex, multidimensional phenomenon shaped by the dynamic interaction of symptom burden, patient-related cognitive and behavioural processes, product characteristics, and health system factors. The findings indicate that suboptimal adherence should not be interpreted solely as a lack of patient motivation, but rather as a reflection of treatment-related challenges, unmet supportive care needs, and limitations in the implementation of nutritional interventions within real-world oncology settings.
Effective improvement of ONS adherence requires a shift from a prescription-focused approach to an implementation-oriented model of nutritional care. Strategies should prioritise proactive symptom management, individualised and preference-based ONS regimens, and structured, continuous follow-up delivered by multidisciplinary teams. In addition, interventions should incorporate behavioural support mechanisms, enhance patient education with practical coping strategies, and actively involve caregivers when appropriate.
System-level factors, including continuity of care, accessibility of services, and reimbursement policies, play a critical role in sustaining adherence and should be integrated into oncology care pathways. Addressing financial barriers and ensuring equitable access to nutritional support are essential for improving outcomes across diverse patient populations.
Future research should focus on the development of standardised and reliable adherence measurement methods, theory-informed and scalable intervention models, and integrated supportive care approaches that combine nutritional support with symptom-directed therapies. Such efforts are necessary to enhance the effectiveness, feasibility, and real-world impact of ONS interventions in cancer care.
Licence
© Author (s), [2026].
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, and unrestricted adaptation and reuse, including for commercial purposes, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
References
-
Xu J, Jie Y, Sun Y, Gong D, Fan Y. Association of Global Leadership Initiative on Malnutrition with survival outcomes in patients with cancer: A systematic review and meta-analysis. Clin Nutr. 2022;41(2):385–394.
-
Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical nutrition in cancer. Clin Nutr. 2021;40(5):2898–2913.
-
Ravasco P. Nutrition in cancer patients. J Clin Med. 2019;8(8):1211.
-
Gomes F, Baumgartner A, Bounoure L, Bally M, Deutz NEP, Greenwald JL, et al. Association of nutritional support with clinical outcomes among medical inpatients who are malnourished or at nutritional risk: An updated systematic review and meta-analysis. JAMA Netw Open. 2019;2(11):e1915138.
-
Wang QC, Yuan H, Chen ZM, Wang J, Xue H, Zhang XY. Barriers and facilitators of adherence to oral nutritional supplements among people living with cancer: A systematic review. Clin Nurs Res. 2023;32(1):209–220.
-
Hubbard GP, Elia M, Holdoway A, Stratton RJ. A systematic review of compliance to oral nutritional supplements. Clin Nutr. 2012;31(3):293–312.
-
Depeint F, Niamba CN, Illner AK, Buche-Foissy C, Branchu J, Younes H, et al. Investigating the modifications of sugar perception and consumption in cancer patients. Nutr Cancer. 2018;70(7):1060–1068.
-
Lidoriki I, Frountzas M, Karanikki E, Katsarlinou E, Tsikrikou I, Toutouzas KG, et al. Adherence to oral nutritional supplementation in gastrointestinal cancer patients: A systematic review of the literature. Nutr Cancer. 2024;76(1):31–41.
-
Wan C, Liu Z, Zhang Y, Liu H, Zhang X, Tang X. Adherence to oral nutritional supplementation in patients after gastrectomy: A mixed methods study protocol. BMJ Open. 2021;11:e044308.
-
Qin L, Xu D, Tian Q, Wu B. Adherence to oral nutritional supplements in patients with gastrointestinal cancer: A mixed-method study. Cancer Nurs. 2022;45(6):E810–E819.
-
Liljeberg E, Nydahl M, Lövestam E, Andersson A. ‘Between foods and medicines’: A qualitative interview study of patient experiences of the meaning and usage of oral nutritional supplements. Appetite. 2022;178:106163.
-
Mayes C. The medicalization of eating and feeding. Health Sociol Rev. 2014;23(1):30–43.
-
Su L, Zhang J, Jia L, Dou W, Li M, Zhang Y, et al. Adherence with oral nutritional supplements and influencing factors in postoperative patients with digestive tract tumors: A cross-sectional study. Support Care Cancer. 2024;32:501.
-
Skinnars Josefsson M, Einarsson S, Seppälä L, Payne L, Söderström L, Liljeberg E. Adherence to oral nutritional supplements: A review of trends in intervention characteristics and terminology use since the year 2000. Food Sci Nutr. 2025;13:e4722.
-
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
-
Lin Y, Fan S, Chai W, Zheng N, Yu D, Yang L, et al. Factors influencing adherence to oral nutritional supplementation in patients with gastrointestinal neoplasms: A mixed methods systematic review. Support Care Cancer. 2025;33:789.
-
Wang Q, Chen Y, Peng Y, Yuan H, Chen Z, Wang J, et al. Preferences of oral nutritional supplement therapy among postoperative patients with gastric cancer: Attributes development for a discrete choice experiment. PLoS One. 2022;17(9):e0275209.
-
Baguley BJ, Arnold H, Bence A, Bryant E, Martino E, Stojanoski K, et al. Systematic review of nutrition interventions in older patients with cancer: A synthesis of evidence and a future research priority. J Geriatr Oncol. 2025;16:102181.
-
Ghias K, Jiang Y, Gupta A. The impact of treatment-induced dysgeusia on the nutritional status of cancer patients. Clin Nutr Open Sci. 2023;50:57–76.
-
Sa-nguansai S, Sae-Lao P, Chaiyasit N. Efficacy of oral nutritional supplement in cancer patients receiving chemotherapy: A systematic review and meta-analysis of randomized controlled trials. Ann Palliat Med. 2024;13(2):260–272.
-
Raso KL, David M, Melton A, Tan SVC, Vardy JL. Bridging the gap between prescription and participation: A systematic review and meta-analysis of factors influencing adherence to prehabilitation in gastrointestinal cancer surgery. Support Care Cancer. 2025;33:973.
-
Liu B, Lin Y, Gui Q, Liu Z, Huang G, Zhao Y, et al. Qualitative study on adherence to oral nutritional supplements in cancer patients: A social cognitive theory perspective. Support Care Cancer. 2025;33:1120.
-
Wang S, Lian W, Lu D, Liu L, Li P, Zhang J. Best practices for home nutritional management in postoperative gastric cancer patients: An evidence summary. BMC Cancer. 2025;25:1399.
-
Liljeberg E, Payne L, Skinnars Josefsson M, Söderström L, Einarsson S. Understanding the complexity of barriers and facilitators to adherence to oral nutritional supplements among patients with malnutrition: A systematic mixed-studies review. Nutr Res Rev. 2025;38(2):407–427.
-
Nunley E, Martinez A, Dains JE. Eligibility and accessibility barriers of patient assistance programs for oral oncolytics in patients with cancer. Clin J Oncol Nurs. 2025;29(1):79–85.