







Double Dilemma: Managing a Sequential Lymphoma (Case Report)
Abstract
Introduction: Sequential lymphoma, characterized by the occurrence of two distinct lymphoma subtypes in tandem within the same patient, presents a unique challenge in diagnosis and management. While transformation from Nodular Lymphocyte-Predominant Hodgkin Lymphoma (NLPHL) to aggressive B-cell lymphomas is well-documented, sequential development of Diffuse Large B-Cell Lymphoma (DLBCL) following Classical Hodgkin Lymphoma (cHL) is exceedingly uncommon, presenting primarily the challenge of cumulative toxicities faced due to different regimens.
Case Report: We present a case of a 25-year-old man initially diagnosed with classical Hodgkin lymphoma (CHL) who subsequently developed diffuse large B-cell lymphoma (DLBCL), following his initial metabolic response to ABVD chemotherapy. Following treatment, he presented disease progression, presenting with a hepatic lesion with diagnosis of CD20 DLBCL, confirming the diagnosis of sequential lymphoma
Management and Outcomes: Due to patients receiving higher cumulative doses of anthracycline therapy, it prompted the decision to consider R-ICE regimen over the traditional R-CHOP regimen primarily due to the risk of increased cardiotoxicity. Better tolerance to the regimen was reported by the patient on the completion of 6 cycles , achieving a complete metabolic response on end-of-treatment PET scan.
Discussion: This case highlights a critical dilemma in managing sequential lymphomas: balancing efficacy against long-term toxicity. The choice of R-ICE over R-CHOP underscores the importance of individualized therapy to mitigate anthracycline-induced cardiotoxicity in young patients. This report adds to the sparse data on this condition and emphasizes the need for consensus guidelines to optimize outcomes in these complex cases.
Introduction
Lymphomas are an extensive group of malignant lymphocytic disorders arising from the proliferation of B- cell, T- cell and natural killer (NK) cell subsets of lymphocytes at different stages of maturation, representing 5% of all malignancies with a combined estimated survival rate of 72%1. Broadly, lymphomas are classified into two major subtypes: Hodgkin Lymphoma (HL) and Non-Hodgkin’s Lymphoma (NHL). The global burden of lymphoma among the population in China from 1990-2019 was evaluated which showed an overall increase of 101,422 new cases comprising 9,468 HL cases and 91,954 NHL cases2,3.
Rarely, a patient can have two distinct lymphoma subtypes within the same anatomical site, called composite lymphomas. An even rarer entity existing within the lymphoma spectrum occurs when a patient develops two different subtypes of lymphoma, in tandems, which is termed as a sequential lymphoma. Recent studies evaluating the incidence of sequential lymphoma cases among Hodgkin Lymphoma patients, recent studies have dwelled into reporting the incidence of transformation of Hodgkin Lymphoma cases into Non-Hodgkin Lymphoma cases, among which the incidence of transformation in Nodular Lymphocytic Predominant Hodgkin Lymphoma (NLPHL) was observed to be greater than it was observed in Classical Hodgkin Lymphoma (CHL)3,4. A retrospective study conducted by Tao et al. of population-based cancer registries within the United States population from 2000-2018 revealed that there were only 116 cases of sequential lymphoma consisting of CHL as a primary malignancy and B-cell lymphoma as a secondary malignancy with a median time of approximately three years between these two cancers5.
Here we report a case of a young gentleman with sequential lymphoma, cHL followed by NHL
Case Presentation
A 25-year-old man presented to the oncology outpatient clinic with a history of consistent significant weight loss, fever, and abdominal pain over the last 6 months. He then underwent a physical examination which revealed a palpable left-sided cervical lymph node.
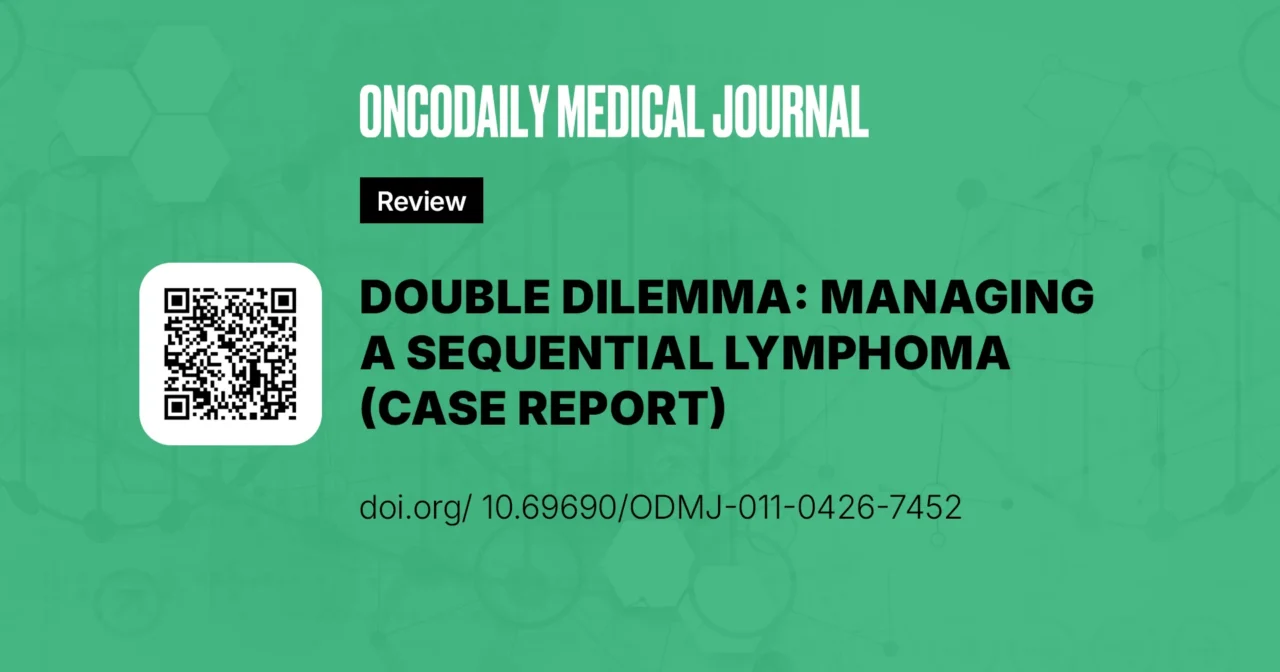
A positron emission tomography (PET) scan was conducted, which showed enlarged cervical, mediastinal, and retroperitoneal lymph node involvement, along with right pleural thickening and pericardial effusion. Bony deposits were also observed within the scan, along with the involvement of liver, mesenteric, omental, and bone marrow. The initial PET scan of the patient is shown in Figure 1. He then underwent an ultrasound-guided biopsy of the omental cervical lymph node. Histopathological examination of the biopsy displayed linear cores of tissue exhibiting a mixed inflammatory background with scattered mononuclear cells. Immunohistochemistry of the biopsy revealed that these atypical cells were negative for leukocyte common antigen (LCA), CD3, and CD15 and were positive for CD30, Pax5, and CD20 (focal positive). Based on the histopathological examination and immunohistochemical test of the resected biopsy, he was diagnosed with classical Hodgkin lymphoma (HL) which prompted the medical team to prescribe him with a treatment regimen of 2 cycles of ABVD (Adriamycin, bleomycin sulfate and vinblastine) treatment.
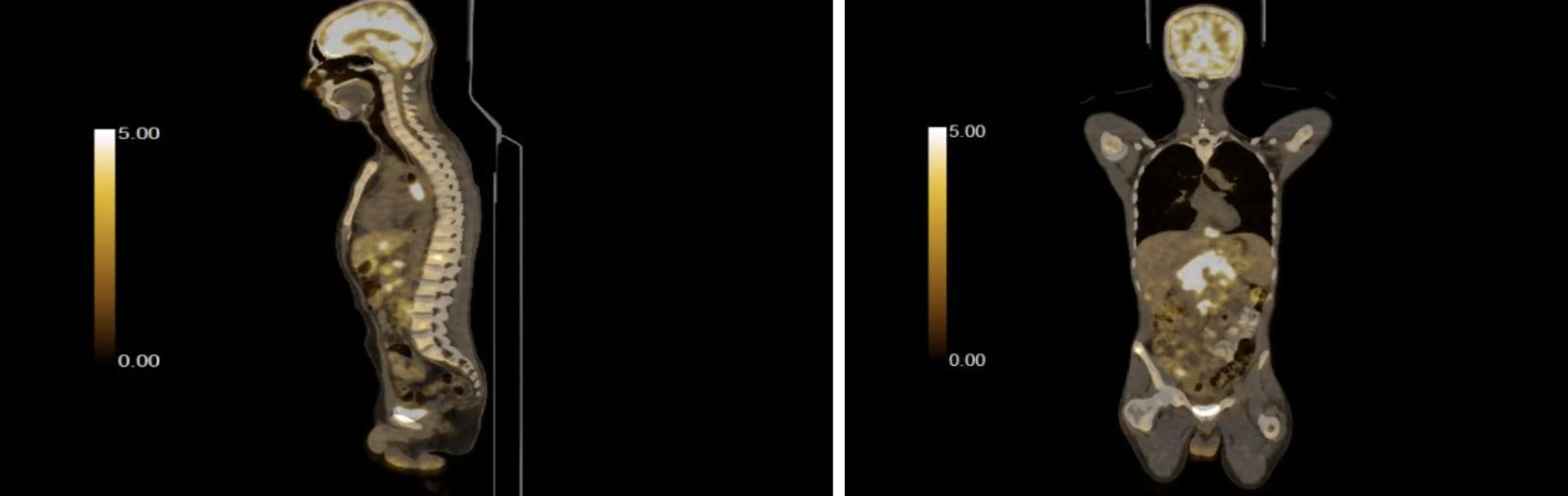
Figure 1: Initial PET scan of the patient with Classical Hodgkin Lymphoma
Two months later, an interim PET scan was conducted which showed complete metabolic response (Deauville score 1), which led the medical treatment to continue with a similar treatment regimen consisting of 4 more courses of ABVD treatment with his end-of-treatment PET scan showed no evidence of disease or it’s progression. The interim PET scan of the patient is shown in Figure 2. Three weeks after the termination of his chemotherapy, he again presented to the outpatient clinic with increased complaints of fever and abdominal pain. Despite his earlier success, the patient’s symptoms worsened, and his PET scan now revealed an interval appearance of multiple hypermetabolic nodal diseases above and below the diaphragm, along with hypermetabolic pleural, peritoneal, splenic, hepatic, stomach, and pancreatic deposits.
Histopathological examination of the biopsy specimen demonstrated linear cores of lymphoid tissue composed of a mixed inflammatory background containing small lymphocytes, eosinophils, and histiocytes with scattered large atypical mononuclear cells morphologically consistent with Hodgkin/Reed-Sternberg (HRS) cells. Immunohistochemical staining revealed that the atypical cells were negative for leukocyte common antigen (LCA), CD3, and CD15, while showing strong positivity for CD30 and weak positivity for PAX5 with focal CD20 expression. These findings were consistent with a diagnosis of classical Hodgkin lymphoma.
Later, histopathological evaluation of the hepatic lesion biopsy demonstrated diffuse infiltration of large atypical lymphoid cells with vesicular chromatin, prominent nucleoli, and abundant cytoplasm. Immunohistochemistry revealed strong positivity for LCA, CD20, CD79a, PAX5, BCL-2, BCL-6, MUM-1, and C-MYC, while CD3 was negative. The morphological and immunophenotypic features supported the diagnosis of diffuse large B-cell lymphoma (DLBCL).The core biopsy for DLBCL is shown in Figure 3.
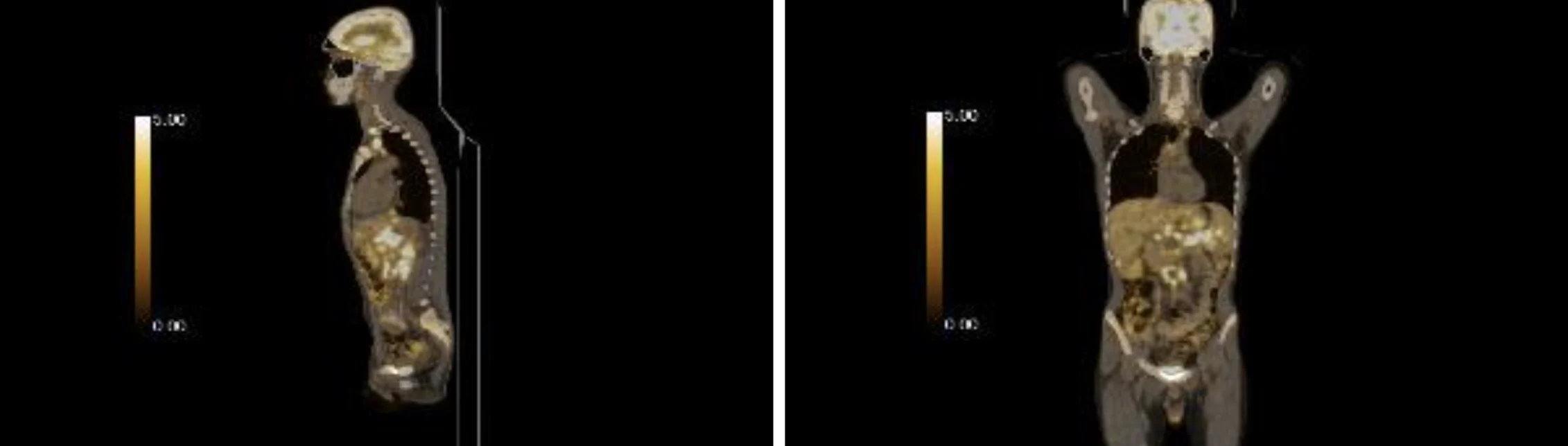
Figure 2: Interim PET scan after the initial treatment
Figure 3:Core Biopsy of the patient with Diffuse Large B-cell Lymphoma. Histopathological findings of the hepatic core biopsy demonstrating diffuse infiltration by large atypical lymphoid cells consistent with diffuse large B-cell lymphoma (DLBCL). Immunohistochemical staining showed strong positivity for CD20, CD79a, PAX5, BCL-2, BCL-6, MUM-1, and C-MYC, confirming B-cell lineage, while CD30 staining was negative, excluding T-cell lymphoma.
The case was discussed in the lymphoma tumor board meeting and keeping in mind his anthracycline chemotherapy over the last 6 months, the board decided to advise him with the R-ICE regimen. To this date, he has completed his six cycles of therapy. An end of treatment PET scan showed a complete metabolic response. The patient is currently on surveillance with history and physical examination every three months.
Discussion
From our review of the existing literature, we observed a huge emphasis to understand the concept of morphosis of nodular lymphocyte–predominant Hodgkin lymphoma (NLPHL) to diffuse large B cell lymphoma (DLBCL), while little to no attention is given to understanding the transformation of classical Hodgkin Lymphoma, which was present within our patient. Most of the studies that dwelled into finding sequential lymphomas of Classical Hodgkin Lymphomas (CHL) are global surveys of the cancer registry which have yielded negative or fewer positive results. A retrospective analysis of the data retrieved from LYSA centers through the LYSA-P and the LYMPHOPATH network from 2000-2018 revealed only one sequential lymphoma case, which showed the transformation of CHL into diffuse large B-cell Lymphoma3. We found only one similar case report that reported the transformation of CHL into DLBCL6, which shows that it is rare in CHL compared to NLPHL, which is common.
The biological mechanisms underlying sequential lymphoma remain incompletely understood. Several hypotheses have been proposed, including treatment-related clonal selection, shared precursor B-cell populations undergoing divergent clonal evolution, and therapy-induced genomic instability7. Molecular studies have demonstrated that some sequential lymphomas originate from a common progenitor clone that later acquires additional genetic alterations leading to histologic transformation8. Additionally, chemotherapy-related immune dysregulation and microenvironmental changes have been proposed as potential contributors to the emergence of secondary lymphoid malignancies9. These observations highlight the biological complexity of sequential lymphoma and underscore the importance of repeat histopathological evaluation when disease relapse occurs after apparent remission.
Although sequential lymphoma remains an uncommon clinical entity, several reports have described the therapeutic approaches and clinical outcomes associated with these cases. Management strategies are generally guided by the histologic subtype of the secondary lymphoma and the patient’s prior treatment exposure. In many cases where aggressive B-cell lymphomas develop following Hodgkin lymphoma, treatment is directed according to standard regimens used for diffuse large B-cell lymphoma, including chemoimmunotherapy regimens such as R-CHOP or alternative salvage regimens when prior therapy limits anthracycline exposure. In a clinicopathological series reported by Aussedat et al., treatment strategies for patients with sequential lymphoma varied considerably and included combinations of chemotherapy, radiotherapy, and hematopoietic stem cell transplantation, highlighting the lack of standardized management guidelines for this condition3. Similarly, a population-based analysis by Tao et al. demonstrated that chemotherapy was the most frequently utilized treatment modality in patients with sequential lymphoma; however, overall outcomes remained heterogeneous and survival rates were inferior compared with those observed in patients with de novo lymphoma5. Isolated case reports have also described the development of diffuse large B-cell lymphoma following Hodgkin lymphoma, emphasizing the rarity of this transformation and the importance of repeat biopsy to establish the diagnosis and guide treatment decisions6. Collectively, these studies underscore the need for individualized treatment strategies that consider prior therapies, cumulative treatment-related toxicities, and the biological characteristics of the secondary lymphoma.
In the contemporary treatment paradigm for relapsed or refractory diffuse large B-cell lymphoma, salvage chemoimmunotherapy followed by consolidation with autologous stem cell transplantation (autoSCT) remains a standard strategy for transplant-eligible patients who achieve chemosensitive disease10. Regimens such as R-ICE, R-DHAP, and R-GDP are commonly utilized as salvage therapies to evaluate treatment responsiveness prior to transplantation11. More recently, chimeric antigen receptor (CAR) T-cell therapy has emerged as an alternative for patients with early relapse or refractory disease; however, autoSCT continues to play an important role in selected patients who demonstrate a favorable response to salvage chemotherapy12. In the present case, the multidisciplinary tumor board initially prioritized systemic salvage therapy with R-ICE due to prior anthracycline exposure and the need to evaluate disease chemosensitivity before considering consolidation strategies.
Despite the rarity of this case, another distinguishing feature of this case is the difference in the medical treatment regimen that was considered in our case. The case was discussed in the multidisciplinary tumor board meeting and the patient was recommended to proceed with R-ICE regimen instead of going with R-CHOP regimen which is usually preferred in B cell lymphoma cases. This decision was taken considering his previous exposure to anthracycline based treatment for CHL (ABVD regimen) as the patient would have surpassed the threshold cumulative dose of doxorubicin, therefore increasing risk of cardiac toxicity. Given the patient’s prior exposure to anthracycline-based chemotherapy (ABVD regimen), the cumulative lifetime dose of doxorubicin was an important consideration. To minimize the risk of treatment-related cardiotoxicity, the multidisciplinary tumor board favored the use of a non-anthracycline salvage regimen, leading to the selection of R-ICE instead of the standard R-CHOP regimen. The case report showed that the patient was given 6 and 3 courses of anthracycline treatment regimen, even after 5 courses of ABVD treatment within the last 2 months6. The reason for going forward with RICE therapy is also been supported by the recent literature which has shown increased cardiotoxic effects of anthracycline drugs, with cardiac events at 7%, 18%, and 65% observed with increased cumulative dose of anthracyclines (150 mg/m2, 350 mg/m2, and 550 mg/m2)13.
Furthermore, other studies have been conducted in the literature, which have primarily emphasized the survival and occurrence of sequential and composite lymphoma, however, there have been few to no studies conducted on specifying the required treatment for reducing the occurrence and complications of sequential lymphoma. A clinicopathological case series conducted by Aussedat et al. reported an incidence of 15 sequential lymphomas, comprising 13 patients with sequential cHl and DLBCL, among which 6 patients were treated with radiotherapy, 4 with allogenous stem cell transplant and 4 with autologous stem cell transplant3. Moreover, poor outcomes were observed with early sequential lymphoma, with no improved outcomes observed with the use of stem cell transplant. Another retrospective conducted by Tao et al. reported the occurrence of sequential lymphoma among 116 patients, with chemotherapy (59.5%) being considered primarily as an initial treatment for these patients. However, similar worse survival rates were observed in this study with a mortality rate of 50.1%5. Given the rarity of sequential lymphoma involving classical Hodgkin lymphoma followed by diffuse large B-cell lymphoma, most available evidence derives from registry-based analyses and small clinicopathological series3,5. Consequently, therapeutic decisions are frequently extrapolated from treatment paradigms used for de novo lymphomas and must be individualized according to prior treatment exposure and patient-specific factors. The present case contributes to the limited literature by highlighting a clinically relevant management challenge; the selection of salvage therapy in the context of prior anthracycline exposure.
Another alternative therapy that was discussed in the tumor board meeting was subjecting patient to an autologous stem cell transplant for the treatment of aggressive DLBCL which was observed in the latest PET scan. Studies have shown the primary use of stem cell therapy as standard procedure for the treatment of multiple myeloma, leukemia, and lymphomas after chemotherapy to reduce the aggravating damage of blood-forming cells, leukocytes, and normal hematopoietic tissue due to increased chemotherapy dosage14,15. Although due to its adverse effects such as tumorigenesis, increased drug toxicity and resistance, we think that there is still a need for further clinical trials and widespread studies to be conducted before its usage in a clinical setting. This case therefore contributes to the limited literature describing sequential transformation of classical Hodgkin lymphoma into diffuse large B-cell lymphoma and highlights the importance of individualized treatment planning in patients with prior anthracycline exposure.
Acknowledgement
None
Declaration of Conflicting Interests: There are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
-
Jamil A, Mukkamalla SKR. Lymphoma. StatPearls. 2023 Jul 17.
-
Liu W, Liu J, Song Y, Wang X, Mi L, Cai C, et al. Burden of lymphoma in China, 1990-2019: an analysis of the global burden of diseases, injuries, and risk factors study 2019. Aging (Albany NY). 2022;14(7):3175.
-
Aussedat G, Traverse-Glehen A, Stamatoullas A, Molina T, Safar V, Laurent C, et al. Composite and sequential lymphoma between classical Hodgkin lymphoma and primary mediastinal lymphoma/diffuse large B-cell lymphoma, a clinico-pathological series of 25 cases. Br J Haematol. 2020;189(2):244-56.
-
Eyre TA, Gatter K, Collins GP, Hall GW, Watson C, Hatton CSR. Incidence, management, and outcome of high-grade transformation of nodular lymphocyte predominant hodgkin lymphoma: Long-term outcomes from a 30-year experience. Am J Hematol. 2015;90(6):E103-E110.
-
Tao Y, Chen H, Liu D, Dai X. Survival among patients with composite and sequential lymphoma between primary mediastinal lymphoma/diffuse large B-cell lymphoma and classical Hodgkin lymphoma: A population-based study. Leuk Res. 2021;111.
-
Balodis A, Anna Pimenova D, Sergey Nikulshin EF, Ginta Balode EF, Hasnere S. Rare Case of Hodgkin Lymphoma Transformation into Diffuse Large B-Cell Lymphoma with Atypical Spread Epidurally, Intradurally and Intramedullary: A Case Report. Am J Case Rep. 2022;23(1):e935014-1.
-
Küppers R. The biology of Hodgkin’s lymphoma. Nature Reviews Cancer 2009 9:1. 2008;9(1):15-27.
-
Pasqualucci L, Dalla-Favera R. Genetics of diffuse large B-cell lymphoma. Blood. 2018;131(21):2307-2319.
-
Coleman R, Zhou Y, Chan A. Adjuvant denosumab in early breast cancer – Authors’ reply. Lancet Oncol. 2020;21(3):e125.
-
Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130(16):1800-1808.
-
Telio D, Fernandes K, Ma C, et al. Salvage chemotherapy and autologous stem cell transplant in primary refractory diffuse large B-cell lymphoma: outcomes and prognostic factors. Leuk Lymphoma. 2012;53(5):836-841.
-
Tun AM, Wang Y, Maliske S, et al. Autologous Stem Cell Transplant in Fit Patients With Late Relapsed Diffuse Large B-Cell Lymphoma That Responded to Salvage Chemotherapy. Transplant Cell Ther. 2024;30(10):1001.e1-1001.e12.
-
Henriksen PA. Anthracycline cardiotoxicity: an update on mechanisms, monitoring and prevention. Heart. 2018;104(12):971-977.
-
Chu DT, Nguyen TT, Tien NLB, et al. Recent Progress of Stem Cell Therapy in Cancer Treatment: Molecular Mechanisms and Potential Applications. Cells. 2020;9(3).
-
Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354(17):1813-1826.