




Prevalence and Associated Factors of Cholelithiasis in Pediatric Sickle Cell Disease Patients at Qatif Health Network, Saudi Arabia
Abstract
Background: This study aimed to estimate the prevalence of cholelithiasis in pediatric SCD patients at Qatif Health Network, Eastern province, Saudi Arabia, besides determining the effect of age, gender, SCD genotype and phenotype, and laboratory markers, along with correlating the impact of co-inheritance of G6PD deficiency, Hydroxyurea treatment, and Ceftriaxone usage on the development of cholelithiasis.
Methodology: An observational, analytic, retrospective, cross-sectional study was performed using a database from Qatif Health Network, following obtaining of approval from the local Institutional Review Board. 108 pediatric SCD patients were included, from ages of 2 to 14 years, regularly attending the pediatric Hematology clinic in the period between January to December 2022. Data was collected using the electronic medical records of the patients, including growth parameters, laboratory investigation results, ultrasound (US) findings, and clinical notes.
Results: The prevalence of cholelithiasis was found to be 26.9%, with a mean age at radiological diagnosis of 12 years (±2.5 years). Female gender was found to be a significant association for cholelithiasis development, with a P-value of 0.038. Total bilirubin level, as well as clinical jaundice, was statistically significant (P-value 0.01) as an association with cholelithiasis. Splenectomy also showed a statistically significant association with cholelithiasis, with a P-value of 0.027. SCD genotype variability, HbS%, Hb level, MCV, platelets, LDH, reticulocytes %, G6PD status, hydroxyurea treatment, and ceftriaxone usage did not show any statistically significant correlation with the development of cholelithiasis.
Conclusion: The prevalence of cholelithiasis in the study among pediatric SCD patients was significant, manifested in the majority of patients with clinical jaundice and elevated total bilirubin levels. Clinical, laboratory indicators, and routine radiological screening are essential for optimal care through early diagnosis and preventing complications, making an appropriate clinical decision for surgical interventions.
Keywords: Sickle cell disease, cholelithiasis, gallstones, hepatobiliary.
Introduction
Sickle cell disease (SCD) is highly prevalent in Saudi Arabia, mainly in the eastern and southern regions of the country. It is an autosomal recessive hematological disease in which the beta globin (Hbβ) of the hemoglobin (Hb) molecules within the normal erythrocytes is substituted by a sickle globin (HbS) that resulting in unstable crescent-shaped red blood cells (RBCs). Under stressful conditions, HbS polymerizes, causing cell sickling, with consecutive damage to the cell membrane. This leads to the generation of rigid and less deformable RBCs that lead to vaso-occlusion, manifested as painful crisis (PVOC), strokes, infarctions, splenic and hepatic sequestrations, acute chest syndrome (ACS), and eventually organ malfunction1.
As the resultant Hb molecule in SCD is unstable, sickle RBCs have a shorter life span compared with the normal RBCs, and SCD patients suffer from chronic hemolysis and anemia. Hyper-hemolysis results in overproduction of bilirubin, which exceeds the liver’s capacity to conjugate, and hence is unable to be excreted in the urine or feces. The excessive bilirubin can subsequently merge with calcium, forming calcium bilirubinate gallstones, which can be asymptomatic or complicated with acute or chronic manifestations2.
Cholelithiasis is a common complication significantly associated with age; the older the age, the higher the prevalence of cholelithiasis. Screening imaging, early diagnosis, and evaluation of complications with appropriate treatment increase survival and improve the quality of life of patients.
In this study, the focus will be directed toward cholelithiasis in pediatric SCD patients. We aimed primarily to estimate the prevalence, associated factors, and complications of cholelithiasis in pediatric SCD patients at Qatif Health Network (QHN). Statistically significant aggravating and alleviating factors will be determined through studying the patients’ demographics, clinical and laboratory detailed parameters, including the effect of age, gender, SCD genotype, HbS%, baseline Hb, MCV, and hemolytic parameters. Also, to correlate the effect of co-inheritance of G6PD deficiency and to evaluate the impact of hydroxyurea (HU) treatment, and the association of ceftriaxone usage on the development of cholelithiasis.
Methodology
An observational, analytic, retrospective, cross-sectional study was performed using a database from QHN after obtaining approval of the local Institutional Review Board (IRB). All pediatric patients from 2 to 14 years of age, attending the Pediatric Hematology clinic in the period between January to December 2022, with SCD as the primary diagnosis, were included in the study. Patients who were on regular exchange or simple blood transfusion programs, those not on regular follow-up, or those who had no abdominal US performed were excluded from the study. Data was collected using the electronic medical records of the patients. It included growth parameters, laboratory investigation results, ultrasound findings, clinical notes written by the consultants during outpatient follow up as well as surgical notes once applicable.
Growth parameters were plotted on the Saudi chart for the specific gender. Routinely done laboratory investigations, including CBC, LDH, reticulocytes percent, liver enzymes, and Hb electrophoresis were recorded, 3-6 months apart, not during ER visits or during hospitalization. Regarding the Hb-electrophoresis, the most recent result was obtained, except for those patients on HU, in which the result preceding the initiation of HU was utilized. All required data was gathered in a survey of Google Forms and subsequently converted to an Excel sheet, where the statistical analysis was performed.
A significant P-value was always considered as 𝛼 ≤ 0.05. At first, the assumption of distribution normality was assessed using histograms and Q-Q plots. As the data was small and was skewed-distributed, the Mann-Whitney and Chi-square tests were used to compare between 2 groups that share one variable, for example, the LDH parameters in patients with/without cholelithiasis.
Ethical approval
This study was approved by the local IRB (QCH-SRECO 27 / 2023), Qatif Health Network ,KSA.
Results
A total of 229 patients were screened, 108 patients were included in the study as they were following regularly in Pediatric Hematology clinic in the period between January to December 2022. Patients on regular simple or exchange blood transfusion, patients not on regular follow up and patients with no abdominal ultrasound (US) done were excluded from the study.
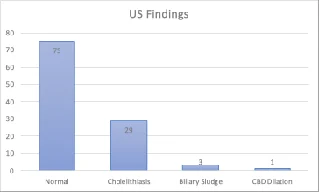
The diagnosis of cholelithiasis can be made basically through US as it is quick, safe, without risk of radiation exposure and with high specificity and sensitivity. The typical findings of gallstones in US is echogenic structures with acoustic shadowing within gall bladder or along the structures of the biliary tract. Out of the 108 patients, 33 patients (30.6%) had gall bladder and bile duct findings, as cholelithiasis in 29 (26.9%) patients, biliary sludge in 3 (2.78%) of them and CBD dilation in 1 (0.9%) patient (Figure 1).
Figure 1. Abdominal US findings of gall bladder and bile duct
Several parameters were tested as dependent variables in correlation with cholelithiasis development, table 1, 2. The mean age in which patients were diagnosed radiologically to have cholelithiasis was found to be approximately 12 years (±2.5 years). Forty three patients were females and 65 patients were males in our study group. Eighteen (41.86%) of the female patients were found to have ultrasound findings, whereas 15 (23.08%) of the male patients were positive, with a statistically significant P-value of 0.038 as female gender to be considered as a significant association for cholelithiasis development.
SCD genotype variability did not show any significance correlation with the development of cholelithiasis, with the majority of patients were homozygous HbSS. The mean HbS %, Hb level, MCV and platelets count exhibited no important correlation with cholelithiasis development.
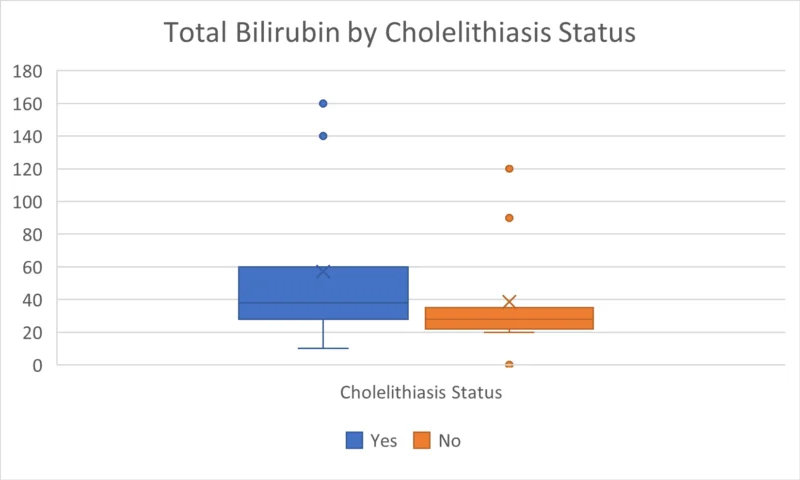
From our data, it was revealed that hemolytic markers LDH and reticulocytes % also showed insignificant correlation with development of cholelithiasis, except for the total bilirubin level which was of statistically significant value. The higher the total bilirubin level, the higher the possibility to develop cholelithiasis with a mean total bilirubin of 48.69 umol/L, compared to 29.53 umol/L in patients without cholelithiasis, with a P-value of 0.00. This correlation was not noticed with the conjugated bilirubin (Figure 2).
Figure 2. The higher the total bilirubin level, the higher the possibility to develop cholelithiasis
In term of clinical characteristics of patients with cholelithiasis, the majority were thriving appropriately to age as 90.9 % of them have their weight between 3rd-95th % for age, and 87.9% have their height between 3rd-95th % for age. Eight (80%) patients manifested clinical jaundice, compared to 2 (20%) patients manifested jaundice without developing cholelithiasis, with a P-value of 0.001. indicating jaundice as a significant association for cholelithiasis. Only two patients (6.1%) were complicated with transaminitis. None of the patients developed pancreatitis.
Splenectomy was done for 7 patients of our study group, 5 (71.4%) of them developed cholelithiasis, while 2 (28.6%) did not, with statistically significant P-value of 0.027 as splenectomy to be considered as a significant association with cholelithiasis.
In correlation to G6PD status, out of 108 included patients, 54 patients were G6PD deficient, 16 (29.6%) patients of them developed cholelithiasis while 38 (70.4%) patients did not. This difference was statistically insignificant with a P-value = 0.835.
Determining the impact of HU treatment, 84 (77.8%) patients in our study were on HU, 28 (33.3%) of them developed cholelithiasis in contrast to 56 (66.7%) participants did not, with statically insignificant p-value of 0.241 for HU treatment to prevent development of cholelithiasis.
Ceftriaxone had been used in 37 (34.25%) patients, 13 (35.14%) of them developed cholelithiasis, and 24 (64.86%) patients did not, with statically insignificant P-value of 0.456 for Ceftriaxone as a significant association for cholelithiasis development.
Thirteen (39.3%) patients with cholelithiasis underwent Laparoscopic cholecystectomy with 0% post-operative morbidity and mortality rate.
Table 1. Tested numerical variables in correlation with cholelithiasis development
| No cholelithiasis | |||
|---|---|---|---|
| Variable | Mean (SD) | Mean (SD) | P-value |
| Age (Months) | 148.03 (26.90) | 118.51 (36.34) | 0.000 |
| HB Electrophoresis , HB S% | 75.95 (6.39) | 71.93 (14.71) | 0.134 |
| Mean MCV fL | 74.33 (9.41) | 69.65 (12.13) | 0.052 |
| HB gm/dL | 9.86 (1.56) | 9.97 (1.30) | 0.701 |
| Platelet | 297.24 (177.96) | 289.77 (136.12) | 0.812 |
| Retics% | 5.22 (2.42) | 5.20 (3.05) | 0.977 |
| LDH U/L | 416.75 (136.36) | 407.12 (148.77) | 0.752 |
| Bilirubin(T) | 48.69 (35.04) | 29.53 (18.11) | 0.000 |
| Bilirubin(C) | 9.36 (4.80) | 10.15 (17.13) | 0.796 |
| ALP | 173.45 (55.46) | 163.99 (50.20) | 0.385 |
| ALT | 29.35 (42.04) | 20.12 (16.39) | 0.103 |
| AST | 45.71 (46.32) | 36.65 (15.53) | 0.132 |
| GGT | 24.07 (38.97) | 19.48 (23.14) | 0.448 |
| if took ceftriaxone , how many times? | 1.85 (3.32) | 2.11 (5.16) | 0.792 |
Table 2. Tested categorical variables in correlation with cholelithiasis development
| Variable | With cholelithiasis | No cholelithiasis | |
|---|---|---|---|
| Counts (%) | Counts (%) | P-Value | |
| Gender | 0.038 | ||
| Female | 18 (41.86%) | 25 (58.14%) | |
| Male | 15 (23.08%) | 50 (76.92%) | |
| SCD genotype | 0.123 | ||
| Hgb S- Beta thalassemia 0 | 1 (11.11%) | 8 (88.89%) | |
| Hgb S- Beta thalassemia 1 | 3 (75.0%) | 1 (25.0%) | |
| Hgb SS | 29 (30.85%) | 65 (69.15%) | |
| Other | 0 (0.0%) | 1 (100.0%) | |
| Percentile for Weight | 0.819 | ||
| 3rd and below | 2 (22.22%) | 7 (77.78%) | |
| 95th and above | 1 (25.0%) | 3 (75.0%) | |
| between 3rd-95th | 30 (31.58%) | 65 (68.42%) | |
| Percentile for Hight | 0.696 | ||
| 3rd and below | 3 (21.43%) | 11 (78.57%) | |
| 95th and above | 1 (25.0%) | 3 (75.0%) | |
| between 3rd-95th | 29 (32.22%) | 61 (67.78%) | |
| Symptoms: | |||
| Jaundice | 8 (80.0%) | 2 (20.0%) | 0.001 |
| Transaminitis | 2 (100.0%) | 0 (0.0%) | 0.091 |
| Pancreatitis | 0 (0.0%) | 1 (100.0%) | 1 |
| Splenectomy | 0.027 | ||
| No | 28 (27.72%) | 73 (72.28%) | |
| Yes | 5 (71.43%) | 2 (28.57%) | |
| G6PD | 0.835 | ||
| Deficient | 16 (29.63%) | 38 (70.37%) | |
| Normal | 17 (31.48%) | 37 (68.52%) | |
| Hydroxyurea | 0.241 | ||
| No | 5 (20.83%) | 19 (79.17%) | |
| Yes | 28 (33.33%) | 56 (66.67%) | |
| Ceftriaxone | 0.456 | ||
| No | 20 (28.17%) | 51 (71.83%) | |
| Yes | 13 (35.14%) | 24 (64.86%) | |
| Cholecystectomy | 0.000 | ||
| No | 20 (21.05%) | 75 (78.95%) | |
| Yes | 13 (100.0%) | 0 (0.0%) | |
| Post-OP complications: | 1 | ||
| No | 33 (30.56%) | 75 (69.44%) | |
| motality | 1 | ||
| Alive | 33 (30.84%) | 74 (69.16%) | |
| Dead | 0 (0.0%) | 1 (100.0%) |
Discussion
Addressing our patients demographics, clinical and laboratory data, the following parameters had shown statistically significant association with development of cholelithiasis:
- Female gender, literature showed no significant association variability in gender with development of cholelithiasis, however in the present study 18 (41.86%) of the female patients were found to have ultrasound findings, with a statistically significant P-value of 0.038 as female gender to be considered as a significant association for cholelithiasis development. This could be otherwise an exaggerated finding due to the relatively small sample size.
- Clinical jaundice, most of the present study population who developed cholelithiasis manifested clinically with jaundice, indicating jaundice as a significant association for cholelithiasis.
- Bilirubin level, the higher the total bilirubin level, the higher the possibility to develop cholelithiasis, as majority of previous studies manifested the significant association of high bilirubin with cholelithiasis formation.
- Splenectomy was observed as a significant association with cholelithiasis, which may indicate development of cholelithiasis in severe complicated phenotype patients.
The prevalence of cholelithiasis is variable in the literature, depending on many cofactors, including age, disease genotype and phenotype, other comorbidities and the medications used in SCD sufferers. In the present study, the prevalence of cholelithiasis was found to be 26.9%, which is comparable to multiple studies performed on Saudi population and estimated to range from 25% to 31% 2,3,4.
The present study showed the mean age in which patients were diagnosed radiologically to have cholelithiasis was approximately 12 years (±2.5 years). In a retrospective study of SCD pediatric patients in a Saudi hospital, the mean age of cholelithiasis was found to be 7 years +/- 3.5 years, with frequency increases from 11.5% in patients <6 years of age to 40.5% in patients 12 years of age and older4. In other national and international studies, cholelithiasis was significantly associated with age, the older the age, the higher the frequency of cholelithiasis2,3,4,5.
The impact of disease genotype on stones formation was addressed in many studies. Within our limited study population, SCD genotype variability did not show any significance correlation with the development of cholelithiasis, with the majority of patients were homozygous HbSS. Correspondingly, cholelithiasis was found in literature to be more frequent in patients with the homozygous Hb SS than HbS/beta or Hb C, these differences were, nonetheless, statistically insignificant3,4.
In the present study, it was observed that the mean HbS % exhibited no important correlation with cholelithiasis development, with statistically insignificant variation in patients with and without cholelithiasis. Howbeit previous studies proved that patients with higher HbS % have a significantly higher incidence of calculi formation with a P-value of 0.0413.
For better understanding of hepatobiliary complications in SCD patients, scientists have studied and many important laboratory markers, including, but not limited to, baseline Hb, MCV, and platelets as well as hemolytic markers and liver function tests. In the present study, in contrast to what is expected, Hb level, MCV and platelets count exhibited no important correlation with cholelithiasis development. Similar to previous studies which reported no significant difference between patients who developed gallstones and those who did not in respect to Hb level3,5,6, while, Webb et al. And Ezer at al reported that children with gallstones had significantly lower total Hb7. Regarding the MCV, AlHawasi et al, found out that patients with cholelithiasis have significantly larger MCV compared to patients without gallstones (MCV= 85 vs. 78, p-value 0.001)3. On the contrary, in an earlier study published in 2010 by Ezer et al, smaller MCV were observed in patients with gallstones8.
From our data, it was revealed that hemolytic markers LDH and reticulocytes % showed insignificant correlation with development of cholelithiasis, except for the total bilirubin level which was of statistically significant value. Some of these studies showed also significant association with high reticulocyte count4,6 and high LDH levels6.
Cholelithiasis can be either asymptomatic or complicated by direct hyperbilirubinemia, transaminitis, acute or chronic cholecystitis, choledocholithiasis, cholangitis, acute pancreatitis, or even acute abdomen, ACS, PVOC, in addition to hepatic and splenic sequestrations.
G6PD Deficiency
As patients with G6PD deficiency have accelerated RBCs turnover under special circumstances and thus may have higher bilirubin levels, some literatures stated that even G6PD deficiency patients without chronic haemolysis still have higher incidence of cholelithiasis than normal individuals which was related to that the UGT1A1 defects that decrease the elimination of bilirubin9. The present study showed no significant association between G6PD deficiency and development of cholelithiasis. In a different study cholelithiasis has been detected in 38% of subjects with chronic hemolytic anemia due to G6PD deficiency, however no epidemiological data available to confirm this hypothesis10.
Hydroxyurea
The effect of HU remains controversial in literature. As the main mechanism of hydroxyurea is to induce production of fetal hemoglobin which has higher affinity for oxygen and thus reduce vulnerability to sickling, it is expected that it reduces the risk of cholelithiasis due to reduced hemolysis and bilirubin production2. Conflicting this hypothesis, the present study did not show this proposed effect, though this finding is really limited by ignorance of the dose, the patient’s compliance and the duration of treatment since initiation. Some studies has found increased incidence of cholelithiasis in patients taking HU, this was however statistically insignificant with P-value of 0.1103. In the study of AlMudaibigh4 statistically significant occurrence of cholelithiasis was found in patients utilizing HU with a percentage of 44% and p-value of 0.018, this finding again was questioned by the adherence of the patients to the medication and the status of gall bladder prior to the use of HU, as the more severe the disease phenotype is, the more the hemolysis and thus the stones formation. On the other hand, Martins, et al.2, has found no association between the use of this medication and the formation of gallstones.
Ceftriaxone
Ceftriaxone is a third-generation cephalosporin that has been frequently used in sever bacterial infections in SCD patient. It is excreted through urine (60%) and bile (40%), it is found to be 20 to 150 times more concentrated in bile than in serum11,12. In general, it is considered to be a safe, commonly used antibiotics in pediatric patients due to its broad spectrum of microbial coverage, long half-life and good penetration to central nervous system. However, it may induce biliary sludge leading to cholelithiasis11,13. This was found to occurs in about 15% – 57% of cases and fortunately majority were asymptomatic and with spontaneous resolution in days to months11,14. The present study showed statistically insignificant association between Ceftriaxone and cholelithiasis development.
Prophylactic Cholecystectomy for patients with asymptomatic gallstones, found incidentally in routine screening, remains an area of debate2,4. This controversy leys from preventing complications caused by chronic gallstones to post-operative complications, such as atelectasis, pneumonitis, ACS, pulmonary infarction, pneumoperitoneum, infections, organ damage, hypothermia, hypovolemia and hematologic instability2,4. In this study, 13 (39.3%) patients with cholelithiasis underwent Laparoscopic cholecystectomy without significant post-operative morbidity or mortality.
Limitations
This study was limited by the small study population and lack of detailed clinical documentations. A larger study population is encouraged to be studied with detailed clinical correlated factors for better assessment of association and outcome. Other limitations includes the study design as it is a single center, retrospective cross sectional study over a relatively short period with selection bias and lack of longitudinal follow-up. Moreover, by excluding patients with no US done, positive cases can be missed. lack of HU compliance data, dose, and the duration of treatment since initiation is another limitation.
Conclusion
The prevalence of cholelithiasis in the study among pediatric SCD patients was significant, manifested in the majority of patients in female gender, post-splenectomy with clinical jaundice and elevated total bilirubin level. Coinheritance of G6PD deficiency, compliance to Hydroxyurea therapy & repeated treatment with Ceftriaxone do not show any significant association with hepatobiliary complication in SCD. Clinical, laboratory indicators and routine radiological screening are essential for optimal care through early diagnosis and preventing complications, keeping an appropriate clinical decision for surgical interventions.
Licence
© Author (s), [2026].
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, and unrestricted adaptation and reuse, including for commercial purposes, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
References
-
Vichinsky EP. Overview of compound sickle cell syndromes. In: UpToDate, Post TW (Ed). UpToDate [Internet]. Waltham (MA): Wolters Kluwer; 2026.
-
Martins RA, Soares RS, De Vito Fb, et al. Cholelithiasis and its complications in sickle cell disease in a university hospital. Rev Bras Hematol Hemoter.2017; 39(1): 28–31.
-
Alhawsawi ZM, Alshenqeti AM, Algarafi AM, Turkistani W. Cholelithiasis in patients with paediatric sickle cell anaemia in a Saudi hospital. J Taibah Univ Med Sci. 2019;14(2):187–192.
-
Almudaibigh AH, Alkasim FA, Ghareeb EF. Prevalence and outcome of cholelithiasis in children with sickle cell disease at King Saud Medical City, Saudi Arabia. J App Hem. 2021;12(4): 203-209.
-
Attalla BI. Abdominal sonographic findings in Sudanese children with sickle cell anaemia. J Diagn Med Sonography. 2010;26:276-80.
-
Kamdem A, Arnaud C, Me×dejel N, Tassel C, Hau I, Pissard S, et al. Gallstones in a newborn-cohort with sickle cell anemia (SCA): Cumulative risk and predictive factors. Blood. 2011;118:513.
-
Webb DK, Darby JS, Dunn DT, Terry SI, Serjeant GR. Gall stones in Jamaican children with homozygous sickle cell disease. Arch Dis Child. 1989;64:693-696.
-
Ezer A, Torer N, Nursal TZ, et al. Incidence of congenital hemolytic anemias in young cholelithiasis patients. World J Gastroenterol. 2010; 16(43): 5457–5461.
-
Huang YY, Huang CS, Yang SS, et al. Effects of variant UDP-glucuronosyltransferase 1A1 gene, glucose-6-phosphate dehydrogenase deficiency and thalassemia on cholelithiasis. World J Gastroenterol. 2005;11(36):5710-3.
-
Meloni T, Forteleoni G, Noja G, et al. Increased prevalence of Glucose-6-phosphate dehydrogenase deficiency in patients with cholelithiasis. Acta Haematol. 1991;85(2):76-8.
-
Cuzzolin L, Oggiano AM, Clemente GM, et al. Ceftriaxone-associated biliary pseudolithiasis in children: do we know enough? Fundam Clin Pharmacol. 2021;35(1):40-52.
-
von Martels JZ, Van de Meeberg EK, Holman M, Ligtenberg JJ, Ter Maaten JC. Pseudolithiasis after recent use of ceftriaxone: an unexpected diagnosis in a child with abdominal pain. Am J Emerg Med. 2013;31:1294.
-
Serdaroglu F, Koca YS, Saltik F, Koca T, Dereci S, Akcam M, Akcam FZ. Gallstones in childhood: etiology, clinical features, and prognosis. Eur J Gastroenterol Hepatol. 2016;28:1468-1472.
-
Bickford CL, Spencer AP. Biliary sludge and hyperbilirubinemia associated with ceftriaxone in an adult: case report and review of the literature. Pharmacotherapy. 2005;25:1389-1395.