




Impact of COVID-19 on the Management of Children with Hepatoblastoma (HB) In Pakistan: A Single Centre Experience
Abstract
Background: The COVID-19 pandemic had grave consequences on healthcare delivery systems, particularly in low middle income countries (LMIC). This study aimed to determine the impact of COVID-19 on clinical presentation and management of children with hepatoblastoma (HB) as compared to pre COVID period.
Methodology: This retrospective cohort study was conducted at the pediatric hematology oncology department by selecting Group A of 24 patients from 2017-2018, pre-COVID-2 years, and Group B of 29 patients during the COVID pandemic 2020 and 2021. Clinical data were collected from record and analyzed by applying the t-test using SPSS version 20.
Results: In group A, 24 children, and in group B, 29 children with hepatoblastoma were enrolled. In both groups, males were predominant with a mean age of presentation of 21-22 months, and the majority presented with raised AFP levels >30,000 ng/ml. In group A, 14 (58%) patients had PRETEXT-II, 2 (8%) had PRETEXT-III unifocal disease, and 2 (8%) patients had vascular invasion. Group B had 9 (31%) patients with pulmonary metastasis, 11 (38%) children with PRETEXT-II, 11 (38%) had vascular invasion, 5 (17%) had PRETEXT-III, and 8 (28%) had PRETEXT-IV disease. Neo-adjuvant chemotherapy was given to 13 (54%) children in group A and 20 (68%) in group B, but surgery was done in 12 (50%) children in group A and only 9 (31%) in group B. Cure rate was 37% with and 64% without abandonment in group A, with a mean follow-up of 30 months, while in group B, 24% with and 43% without abandonment, with a mean follow-up of 26 months. Treatment abandonment was > 40% in both groups, and the mortality rate was 25% in group A and 20% in group B.
Conclusion: COVID-19 significantly impacted children with hepatoblastoma, leading to more advanced, metastatic, and unresectable disease, posing them with a dismal prognosis.
Keywords: COVID-19, Pandemic, Hepatoblastoma, Pediatric Oncology, Low and Middle income countries (LMIC).
Introduction
The COVID-19 pandemic has significantly disrupted health care systems globally, with particularly severe implications in low and middle-income countries (LMICs), including Pakistan1. These disruptions have hindered the prompt diagnosis and treatment of several diseases, especially pediatric cancers. Although the overall incidence of COVID-19 was low among pediatric cancer patients, with most cases occurring in those with hematological malignancies (e.g., leukemia/lymphoma) rather than solid tumors, and the majority presented with mild disease2,3.
The profound impact of the pandemic on pediatric oncology underscores the critical need to investigate its consequences on the management of pediatric cancers. Key challenges included healthcare service disruptions due to lockdowns, patients’ fear of visiting hospitals, reallocation of resources, and suspension of non-urgent services. In addition, travel restrictions further exacerbated access barriers, resulting in delays in referrals and timely treatment. Furthermore, ensuring staff safety and managing workforce disruptions were major challenges in maintaining hospital operations during the pandemic. The limited availability of pediatric surgeons due to their own health concerns and prioritizing surgical services for emergencies led to interruptions in planned tumor surgeries, thus impacting surgical service delivery4,5.
This study aims to evaluate the COVID-19 pandemic’s impact on the clinical presentation, management, and outcomes of children with hepatoblastoma, comparing these factors to the pre-COVID period at our institution.
Methodology
This retrospective cohort study was conducted in the Department of Pediatric Hematology-Oncology, the Children’s Hospital, and the University of Child Health Sciences Lahore, Pakistan. The study aimed to evaluate the impact of the COVID-19 pandemic on the management of hepatoblastoma by comparing the clinical profiles and treatment outcomes of children diagnosed with hepatoblastoma during two defined study periods: the pre-COVID-19 span (2017-2018) and the COVID-19 pandemic/immediate post-pandemic period (2020–2021).
The study included 53 children aged 0-18 years with a histologically or radiologically confirmed diagnosis of hepatoblastoma who presented to the department during the pre-defined study periods:
- Group A (Pre-COVID-19 cohort): Included 24 patients with HB who presented during January 2017 to December 2018.
- Group B (COVID-19 cohort): Included 29 patients with HB who presented during January 2020 to December 2021.
After getting approval from the institutional review board, data were collected from hospital medical records, including radiology reports, histopathology findings, and treatment charts. The variables of interest included: demographic details: age at diagnosis, gender, and disease characteristics such as presenting symptoms, baseline PRETEXT-stage, alpha-fetoprotein (AFP) levels, and risk stratification group. Treatment details, including the type of chemotherapy protocol administered and the surgical resection status, were also documented. The data regarding follow-up of both groups were recorded from the outpatient departments’ records and by calling them on phones. In group A, the mean follow up of 30 months, while in group B, the mean follow-up duration was 26 months from the date of diagnosis.
At our institution, the diagnosis of hepatoblastoma was established on the basis of elevated serum alpha-fetoprotein (AFP) levels and radiographic detection of a hepatic mass on triphasic abdominal computed tomography (CT), along with histopathological confirmation obtained from needle biopsy specimens. Contrast-enhanced CT of the chest was performed in all cases to exclude pulmonary metastases. Risk stratification was carried out according to the SIOPEL (International Childhood Liver Tumours Strategy Group)–based CCLG guidelines, and subsequently received neoadjuvant chemotherapy according to risk group.
Following completion of preoperative chemotherapy, all cases were reviewed in the institutional multidisciplinary tumor board, and surgical resectability was assessed by the pediatric surgical team at our center. Outcome measures were assessed in terms of overall survival (OS), event-free survival (EFS), relapse rate, treatment abandonment, and mortality. The OS duration was defined as the interval between the time of diagnosis and the time of death, and event-free survival (EFS) as the interval between the time of diagnosis and the time of the first occurrence of tumour progression, relapse, or death, whichever occurred first.
Data were entered and analyzed using SPSS version 20. Continuous variables (e.g., age, AFP levels) were expressed as mean ± standard deviation (SD) and compared using the independent sample t-test. Categorical variables (e.g., sex, tumor stage, treatment abandonment) were expressed as frequencies and percentages and compared using the Chi-square test. A p-value < 0.05 was considered statistically significant. Survival analysis was performed using the Kaplan–Meier method and the Log-Rank Test to compare survival.
Results
Patient demographics
A total of 53 patients diagnosed with HB were enrolled in this study, comprising 24 children in Group A and 29 in Group B. Male predominance was observed in both groups, i.e., 16 (66%) and 23 (79%) in the A and B groups, respectively. The children’s age on presentation ranges from 1-120 months in both group with mean ages of 21.4 months in group A and 22.8 months in group B, and median age was 12 months and 16 months in groups A and B, respectively. (Table 1)
Table 1: Clinical Characteristics
| Category | Sub-category | Group-A n=24 | Group-B n=29 |
|---|---|---|---|
| Mean Age | Months | 21m | 22 m |
| Gender | Male | 16 (66%) | 23 (79%) |
| Gender | Female | 8 (33%) | 6 (20 %) |
| AFP level | >30000 ng/ml | 18 (75%) | 18 (62%) |
| Risk stratification | Standard Risk | 8 (33% ) | 6 (21%) |
| Risk stratification | High Risk | 4 (17%) | 7 (24%) |
| Risk stratification | Very High Risk | 0 | 9 (31%) |
| Outcome | Abandonment upfront | 8 (33%) | 10 (35%) |
| Outcome | Lost to follow up | 2 (8%) | 3 (10%) |
| Outcome | Cure rate without Abandonment | 64% | 43% |
Disease Characteristics and Pre-Text Staging
The majority of children with HB, 18 (75%) in group A and 18(62%) in group B, presented with raised AFP levels of >30,000 ng/ml, while only one patient had less than 100 ng/ml in group B. (Table 1)
In group-A most of the patients, 14 (58%), had PRETEXT-II disease, while 2 (8 %) patients had PRETEXT-III unifocal disease, 2 patients (8%) had vascular invasion, and only one patient had extra-hepatic disease without any pulmonary metastasis. Conversely, in group B 9 (31%) children presented with pulmonary metastasis, 11 (38%) with vascular invasion, 11 (38%) with PRETEXT-II, 5 (17%) with PRETEXT-III, and 8 (28%) children with PRETEXT-IV multifocal disease.
Liver’s right lobe involvement was observed in 46% patients in group A and 41% in group B. Left lobe involvement was noted in 8% patients in group A and 14% in group B, while multifocal disease involving both lobes was seen exclusively in 28% patients of group B. (Figure 1)
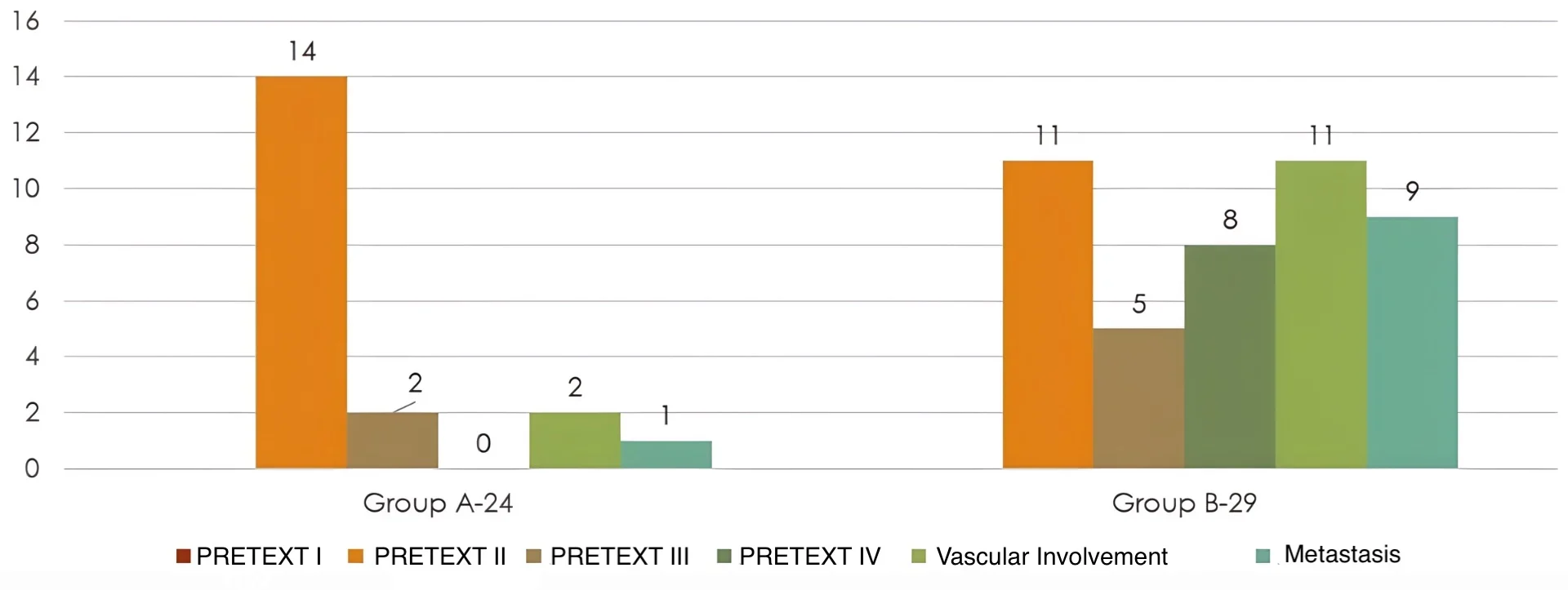
Fig. 1. The graphs show the PRETEXT staging in patients in Group 1 and Group 2.
In Group A, histopathological analysis revealed 50% with non-specific findings, 25% of the cases with fetal histology, 4% with epithelial type, whereas in 21% of patients, biopsy was either not done or unavailable. In Group B, 52% of children exhibited non-specific histology, 14 % had fetal type, 10% both epithelial and mixed type,s and 3.5% small cell undifferentiated type.
Risk stratification was identified in 33% of patients with standard risk and 29% with high risk disease in group A, whereas group B comprised 21% standard risk, 24% high risk, and 31% very high risk disease cases. Neo-adjuvant chemotherapy was administered according to the assigned risk group category, in 13 (54%) patients in group A and 20 (68%) in group B. Surgical resection was achieved in 12 (50%) patients in group A, while in group B, 9 patients (31%) underwent surgery followed by adjuvant chemotherapy. However, 8 patients (28%) continued to have unresectable disease despite preoperative chemotherapy.
Outcome
The cure rate was 37% with and 64% without abandonment in group A, with a mean follow-up of 30 months, while in group B, 24% with and 43% without abandonment, with a mean follow-up of 26 months. Treatment abandonment rate was high in both groups, i.e., 41% and 44% in groups A and B, respectively, and among them majority had upfront abandonment, 33% (group A) and 34% (group B) before starting any treatment. In group A total of 6 (25%) children died, and among them, 2 died before any treatment, 2 from chemotherapy toxicity, 1 due to postoperative complications, and one with relapsed disease. In group B 5 (20%) children died 2 due to relapse disease, 1 with progressive disease, and 2 with treatment complications. Relapse rate was almost the same, 8% in group A and 7% group B. (Figure 2)
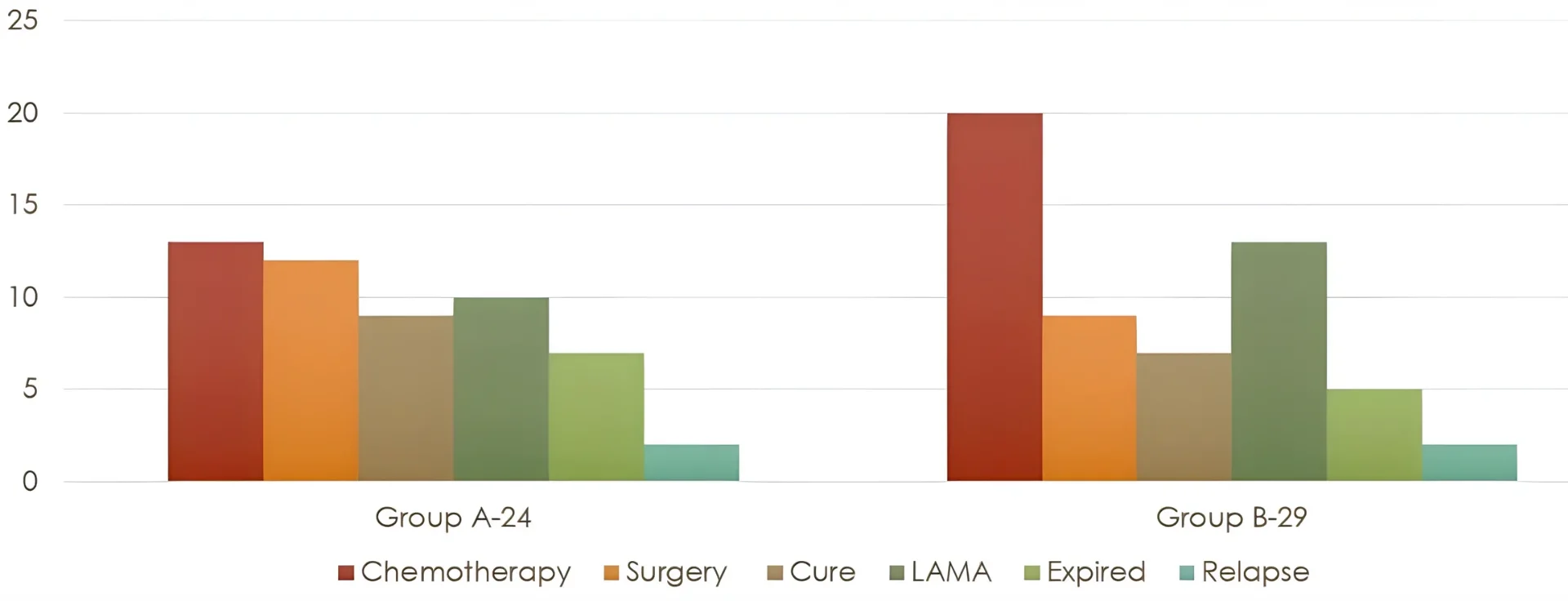
Fig. 2. Graph showing the outcomes.
The Kaplan–Meier survival analysis compared the survival experience of pre-COVID and post-COVID patient groups over a 24-month follow-up period. The mean survival time for pre-COVID patients was 15.4 months, while for post-COVID patients it was 13.5 months, reflecting a shorter average survival duration among post-COVID patients. The log-rank (Mantel–Cox) test showed no statistically significant difference between the two survival curves (p value of 0.523). The observed disparity in survival outcomes was not strong enough statistically to confirm that COVID-19 status had a measurable impact on survival time within this sample. (Figure 3)
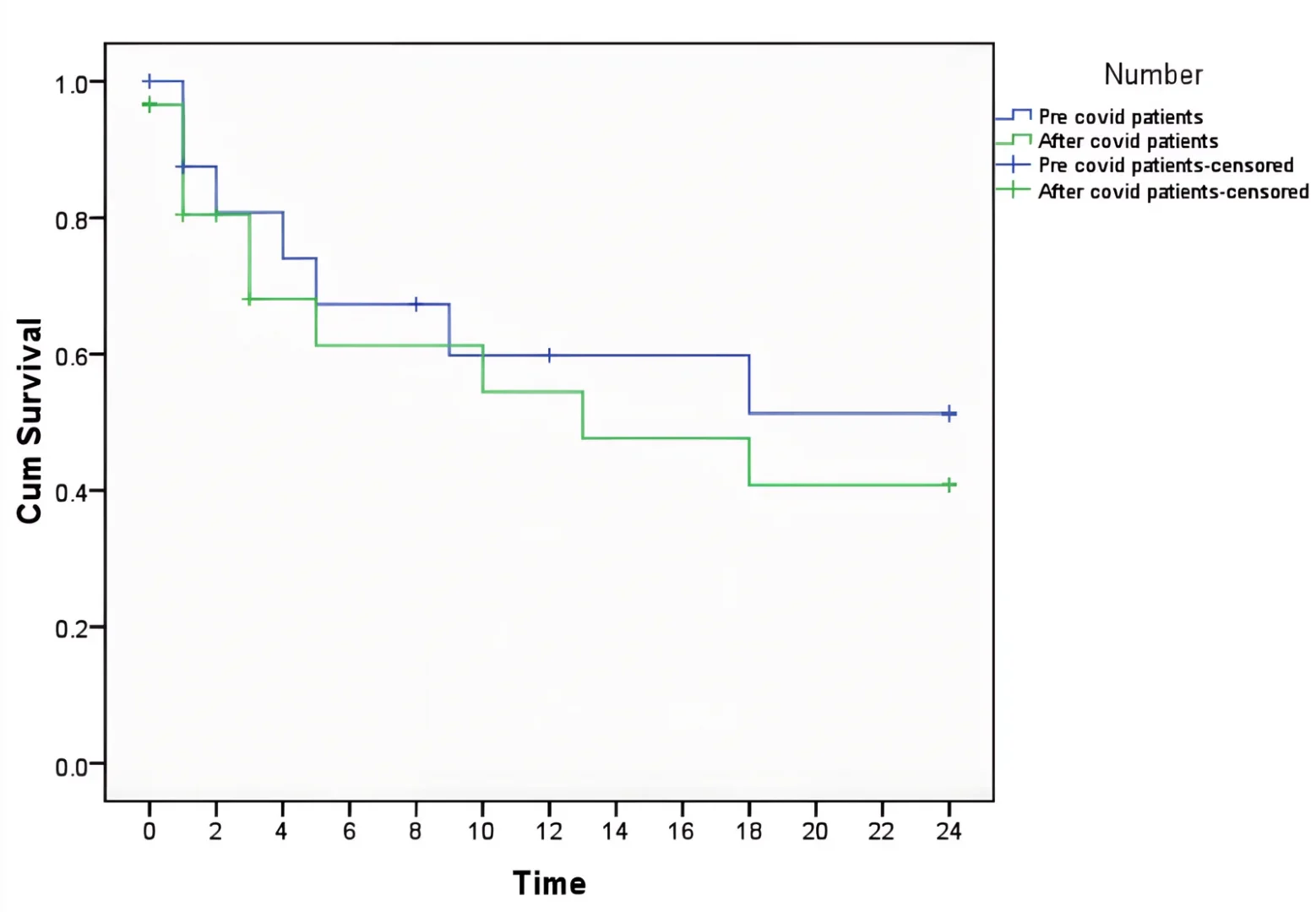
Fig. 2. Survival functions.
Discussion
The COVID-19 pandemic has been one of the most significant global health crises of the 21st century, causing unprecedented disruption to healthcare systems. Its adverse effects were especially severe in low- and middle-income countries (LMICs), where diverted resources, lockdowns, and limited access to specialized care further strained fragile health infrastructures. Pediatric oncology, which relies heavily on resources, was deeply impacted, with delays in diagnosis, interruptions in therapy, and challenges in providing supportive care5,6,7.
The pandemic significantly disrupted the management of hepatoblastoma (HB) in resource-limited settings, exposing multiple weaknesses in healthcare delivery. Our findings align with global reports, which show that delays in diagnosis and treatment disruptions during the pandemic led to more advanced disease at presentation and worse outcomes in children with HB. Regarding age of presentation, gender, and baseline AFP levels, no significant difference was observed between the two groups. However, in our study in group B, children diagnosed during the pandemic were more likely to have high-risk features, such as pulmonary metastases, vascular invasion, and multifocal tumors corresponding to PRETEXT III and IV disease, compared to those diagnosed before the pandemic. This pattern highlights the indirect effects of pandemic-related restrictions, like lockdowns, reduced healthcare access, and interrupted referral pathways, all of which are known to delay cancer detection and treatment8.
The pandemic placed enormous pressure on healthcare systems in many developing countries, causing delays in diagnosis, reduced surgical capacity, and interruptions in ongoing care for children with hepatoblastoma. Since early detection and timely surgical removal are crucial for positive outcomes, these delays can drastically worsen prognoses. During the pandemic, many centers, including our center, shifted their therapeutic approaches toward increased and prolonged use of neoadjuvant chemotherapy where timely surgical resection was not possible due to non availability of surgeons. At the same time, the rates of definitive surgical resection declined as depicted by a smaller number of curative surgical resections in our second cohort (group-B), reflecting limited surgical resources and barriers to timely operative management5,9,10.
The strain on health systems from COVID-19 resulted in delayed diagnoses, decreased surgical capability, and interruptions in continuous care for children with hepatoblastoma. Because early detection and immediate surgical removal are vital for curing hepatoblastoma, delays in diagnosis or definitive surgery significantly impair prognosis8.
Global reports, including an audit from a major pediatric oncology center in Turkey, have shown substantial declines in outpatient visits, inpatient admissions, and essential diagnostic and therapeutic procedures, such as surgery, chemotherapy, and radiotherapy, during the COVID-19 period. These disruptions reveal how strained healthcare resources and institutional limitations led to postponements of definitive surgical interventions and an increased reliance on neoadjuvant or alternative nonsurgical treatments11. Our current study further confirms this pattern, with more metastatic disease at presentation, lower resection rates, and worse outcomes for children with hepatoblastoma during the pandemic compared to the pre-COVID period.
During the pandemic, children more often presented with advanced hepatoblastoma and had limited access to potentially curative surgeries. This, combined with delayed diagnoses, resulted in poorer survival outcomes and higher rates of treatment abandonment. Surgical capacity was globally reduced during COVID-19, disproportionately impacting LMICs, where prompt surgery is already tricky9. In our cohort, two-year survival rates decreased during the COVID period, and abandonment rates increased, consistent with findings from international pediatric oncology studies.
Socioeconomic challenges and mobility restrictions during lockdowns further contributed to treatment discontinuation, a pattern commonly seen in LMICs. Although crude mortality appeared slightly lower during the pandemic, this reflects shorter follow-up periods rather than actual improved survival 4,5,6,9,10.
Conclusion
In conclusion, the pandemic has exacerbated existing disparities in pediatric oncology, impeding progress toward improved childhood cancer outcomes and underscoring the vulnerability of children with HB in resource-limited settings. Ultimately, the pandemic has highlighted the urgent need for robust and adaptable healthcare systems capable of sustaining essential services and protecting vulnerable populations during worldwide emergencies.
Conflict of interests: The authors declare no conflict of interests.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
License
© The Author(s) 2026.
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, and unrestricted adaptation and reuse, including for commercial purposes, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
References
-
Ali N, Ghalibafian M, Sykes-Martin K, et al. Impact of COVID-19 pandemic on delivery of pediatric radiotherapy: a critical review. Pediatr Blood Cancer. 2023 Aug;70(8):e30446.
-
Sundberg E, Georgantzi K, Langenskiöld C, et al. Low numbers of COVID-19 in Swedish pediatric oncology patients during the first pandemic year despite an open society. Pediatr Blood Cancer. 2022 Oct;69(10):e29750.
-
Shaheen N, Wali RM, Saeed H, et al. Acute morbidity and mortality analysis of COVID-19 in children receiving cancer treatment. J Coll Physicians Surg Pak. 2021 Jan;31(1):S83–S86.
-
Meena JP, Kumar Gupta A, Tanwar P, et al. Clinical presentations and outcomes of children with cancer and COVID-19: A systematic review. Pediatr Blood Cancer. 2021 Jun;68(6):e29005.
-
Seth R, Das G, Kaur K, et al. Delivering pediatric oncology services during a COVID-19 pandemic in India. Pediatr Blood Cancer. 2020 Dec;67(12):e28519.
-
Graetz D, Agulnik A, Ranadive R, et al. Global effect of the COVID-19 pandemic on paediatric cancer care: A cross-sectional study. Lancet Child Adolesc Health. 2021 May;5(5):332–340.
-
Noun P, Farhat M, Khalife H, et al. Impact of COVID-19 on clinical outcomes and care delivery in pediatric oncology patients in Lebanon in 2020–2023: a retrospective study. Front Pediatr. 2025 Jul 9;13:1608740.
-
Xu H, Zhou Y, Sun R, et al. A narrative review of the challenges and countermeasures in hepatoblastoma management during COVID-19 epidemic. Transl Pediatr. 2020 Dec;9(6):840-8.
-
Majeed A, Wright T, Guo B, et al. The global impact of COVID-19 on childhood cancer outcomes and care delivery: A systematic review. Front Oncol. 2022 Apr 7;12:869752.
-
Saab R, Obeid A, Gachi F, et al. Impact of the coronavirus disease 2019 (COVID-19) pandemic on pediatric oncology care in the Middle East, North Africa, and West Asia region: a report from the Pediatric Oncology East and Mediterranean (POEM) group. Cancer. 2020 Sep 15;126(18):4235-45.
-
Kutluk MT, Ahmed F, Kirazlı M, et al. The effect of the COVID-19 pandemic on paediatric cancer care: lessons learnt from a major paediatric oncology department in Turkey. Ecancermedicalscience. 2021 Jan 14;15:1172.