




Enhancing Palliative Care Through Simulation-Based Workshops for Effective Symptom Management
Abstract
Introduction: Effective symptom management is a key component of palliative care, aiming to alleviate suffering and improve the quality of life for individuals with chronic illnesses. However, healthcare providers often face challenges in managing symptoms such as pain, dyspnea, nausea, constipation, and agitation due to limited competence, insufficient training, and lack of confidence. Therefore, simulation-based workshops efficiently bridge the gap between theory and practice, promoting better symptom management.
Methodology: A quasi-experimental, mixed-methods study was conducted to evaluate a four-hour workshop, structured using the Plan-Do-Study-Act (PDSA) framework. Thirty-three registered nurses participated in didactic sessions, case-based discussions, high-fidelity simulations, and structured debriefings. A 15-item pre- and post-workshop questionnaire assessed knowledge, while a post-intervention 5-point Likert-scale survey, along with two open-ended questions, gathered qualitative feedback on learning outcomes and interprofessional collaboration.
Results: Participants showed a significant improvement in knowledge scores, increasing from 58.4% ± 10.6 to 87.3% ± 8.9 (p < 0.001), indicating a 70% relative gain. Furthermore, 75% of participants reported enhanced interprofessional collaboration and decision-making based on Likert-scale feedback, highlighting the role of simulation in fostering interprofessional synergy and improving clinical decision-making in palliative care.
Conclusion: Integrating clinical knowledge with experiential learning equips nurses to confidently manage complex patient needs, ensuring dignified and patient-centered care. To ensure sustainability, regular refresher courses and incorporation of these workshops into ongoing professional development programs are recommended. Healthcare institutions should also adopt a palliative curriculum and encourage participation to promote high-quality palliative care delivery.
Keywords: Palliative care nursing, Simulation-based Learning, Symptom Management.
Introduction
Symptom burden remains one of the most significant challenges faced by patients with chronic and life-limiting illnesses, despite advances in modern medical therapies and specific treatments. Managing complex symptoms requires comprehensive, coordinated care and clinical expertise. This ongoing challenge is illustrated in the following clinical scenario. A 62-year-old female patient presented to the outpatient palliative clinic with complaints of dyspnea, fatigue, pedal edema, and a persistent cough. She had been diagnosed with congestive heart failure six years earlier. At this visit, the oncologist provided conservative management and referred her to the palliative care team to incorporate a multidisciplinary approach. This case scenario reflects the growing need for comprehensive palliative care services for patients living with chronic, progressive, and symptom-burdening illnesses.
Palliative care focuses on alleviating suffering and optimizing the quality of life for patients with chronic or serious illnesses. In addition to this, it is a comprehensive approach that addresses physical, psychosocial, emotional, and spiritual needs. Among these domains, effective symptom management remains a cornerstone of physical care. Managing symptoms such as pain, dyspnea, nausea, constipation, and agitation is essential for ensuring patient comfort and well-being1,2,3,4. A key component of delivering quality palliative care in terms of symptom management is the healthcare team’s responsibility which includes physicians, nurses, pharmacists, nutritionists, physiotherapists, and other allied professionals. Yet the most crucial role in assessing and implementing symptom management plans is played by nurses as they provide direct care and conduct assessments on patients on an ongoing basis; Despite their central role in symptom assessment and management, nurses frequently report feeling inadequately prepared to manage complex palliative care scenarios. Several factors contribute to this gap. Limited structured training in palliative care during undergraduate education, insufficient continuing professional development opportunities, and heavy clinical workloads often restrict time available for skill development. Additionally, organizational and financial constraints may limit investment in specialized palliative education programs, particularly in resource-constrained healthcare settings. These challenges contribute to reduced confidence in symptom management, communication during end-of-life discussions, and nterdisciplinary coordination2,3,4,5,6. Addressing these systemic and educational barriers is essential to strengthening palliative care delivery and improving patient outcomes.
To address these gaps in training and confidence, simulation-based learning (SBL) has emerged as an effective method that offers a safe, experiential, and replicable environment to practice clinical skills and interprofessional teamwork without putting patients at risk. Furthermore, SBL offers hands-on practice in realistic scenarios that closely mimic real-life clinical situations. Recent studies demonstrate that SBL enhances knowledge, communication, and self-efficacy among clinicians in palliative care contexts3,4,5,6,7,8.
This study aimed to evaluate the impact of a recently introduced 4-hour simulation-based workshop on the knowledge, competencies, and clinical skills of nurses in Home Health Services (HHS) of Aga Khan University Hospital in managing palliative care symptoms during a 4-hour workshop. This represents the first structured implementation of a simulation-based palliative care workshop in the HHS unit. The objectives of the research were to improve evidence-based knowledge through theoretical sessions, develop practical and clinical skills through simulation exercises, foster interprofessional teamwork and collaboration through case studies, and strengthen critical thinking and decision-making in symptom management using scenario-based activities.
Methodology
Study Design
A quasi-experimental, mixed-methods design was employed to evaluate the effectiveness of a simulation-based workshop on nurses’ knowledge, confidence, and interprofessional collaboration in palliative symptom management. This design allowed for both quantitative assessment of knowledge gains and qualitative exploration of participant experiences, thus providing a comprehensive evaluation of the interventions based on assessment and scenario-based mock drills. Recent studies support the value of such approaches: for example, a quasi-experimental simulation program using standardized patients significantly improved nursing students’ end-of-life care knowledge and confidence5,7. Similarly, virtual clinical simulation has been shown to enhance nursing students’ palliative care knowledge, ability, and attitudes in a mixed-methods context³. Moreover, a scoping review of SBL in postgraduate palliative nursing education confirmed that simulation fosters interprofessional teamwork and critical thinking⁴. Further, recent mixed-methods research has demonstrated that simulation enhances self-efficacy among nursing students, particularly when combined with qualitative reflections⁹. Finally, systematic reviews of SBL in nursing education also show consistent gains in knowledge and skills across diverse settings⁶.
Although the workshop was structured using the Plan–Do–Study–Act (PDSA) framework to guide implementation and iterative refinement, the PDSA cycle served as an operational and quality improvement model for delivering the educational intervention rather than defining the research design. The evaluation component was prospectively developed with predefined outcome measures, statistical analysis, and mixed quantitative–qualitative data collection to contribute to the evidence base on simulation-based palliative care education among practicing nurses.
Setting and Participants
The study was conducted at HHS, Outreach Medical Services of the Aga Khan University Hospital, Karachi, Pakistan. The target population consisted of 33 registered nurses actively involved in palliative care provision. The sample size was determined based on feasibility, reflecting the number of nurses available and nominated by the HHS unit during the study period. Given the educational nature of the intervention, no formal power analysis was undertaken. A convenience sampling technique was employed, whereby all eligible nurses meeting the inclusion criteria were invited to participate.
The participating nurses were registered nurses employed within the HHS unit of Outreach Medical Services. In this setting, nurses provide direct patient care in patients’ homes and are responsible for ongoing clinical assessment and symptom management for individuals with chronic and life-limiting illnesses. Their roles include conducting routine symptom screening and day-to-day pain assessments, monitoring vital signs and other distressing symptoms, administering prescribed medications, performing wound care, providing patient and family education, and communicating changes in patient condition to physicians and the interdisciplinary team. In addition to this, nurses also support family caregivers through counselling, coordination of care, and end-of-life communication when required. Given their frontline role in symptom identification and intervention within a home-based setting, strengthening their competence in palliative symptom management is critical for ensuring safe and patient-centered care.
Inclusion criteria were:
- Possession of a valid registered nurse (RN) license.
- Active employment within the HHS unit.
- Current clinical role involving potential responsibility for managing or handling palliative care patients
Exclusion criteria included:
- Prior participation in simulation-based palliative care training within the past 12 months.
The workshop was conducted as part of professional development and capacity-building for HHS nurses. Participation was voluntary for all nominated nurses, and those who attended received a departmental certificate. Completion of pre- and post-workshop assessments was required as part of this training. However, use of the assessment data for research purposes was voluntary, and informed consent was obtained prior to data collection. No additional incentives were provided.
Workshop Description
Although SBL is increasingly used in nursing education, most studies focus on students rather than practicing nurses. SBL is particularly important for practicing nurses who provide direct patient care. It offers a safe environment to refresh clinical skills, integrate updated evidence-based knowledge, and build confidence in managing complex patient situations.
To address the required needs to conduct this workshop, this study implemented a four-hour PDSA-guided workshop for registered nurses at a tertiary outreach service, focusing on symptom management and evaluating changes in knowledge, confidence, and perceived interprofessional collaboration. To conduct the workshop, it requires a process flow that has a strategic plan, interventions, and results, so this tool is an influential outline to conduct research-based workshop that provides an Additionally, few studies incorporate SBL within structured quality improvement framework to develop, implement, and test the outcomes and refine the process, such as the Plan-Do-Study-Act (PDSA) cycle, which allows interventions to be refined based on systematic evaluation.
A recent review found that SBL in postgraduate palliative nursing education enhances teamwork, communication skills, and professional growth. However, the review also noted limited attention to symptom management and a predominance of student-focused research, highlighting the need for studies targeting practicing clinicians3,4,5,6,7,8,9.
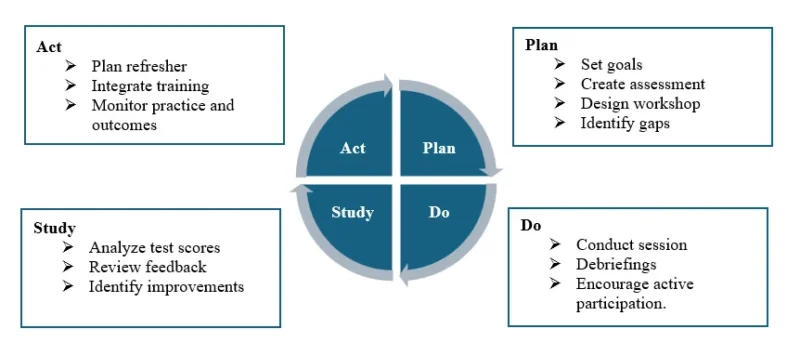
The workshop was structured around the PDSA cycle. In the planning phase, specific goals were established:
- Improve nurses’ evidence-based knowledge by at least 20%, as measured by pre- and post-tests within one month.
- Provide each nurse with at least two hands-on simulation experiences to enhance clinical skills.
- Strengthen critical thinking and decision-making in palliative care by achieving at least 80% accuracy in simulated patient scenarios.
Fifteen-item multiple-choice tests were developed to assess knowledge before and after the workshop. Simulation scenarios were designed to give participants practical experience managing common palliative care symptoms. The workshop content included palliative care principles, symptom assessment and management, basic nursing interventions, and documentation practices. Necessary logistics, including patient actors and materials, were arranged to ensure realistic and effective practice.
During the Do phase, sessions combined lectures with simulation exercises. Nurses actively participated in scenarios, performing interventions appropriate to the patient’s condition. Each scenario concluded with debriefing using the Gather, Analyse and Summarize method, and participants completed the Feedback and Self-Efficacy Questionnaire (SEQ) to share their reflections. This combined approach aligns with findings, that demonstrated that integrating lectures with simulation produced greater knowledge gains in hospice and palliative care compared to simulation alone⁸.In the study phase, assessment scores and participant feedback were analysed to identify strengths and areas for improvement in the workshop design and delivery.
In the Act phase, strategies were developed to sustain and expand the workshop’s impact. These included refresher workshops, integration of simulation into ongoing palliative care training, and monitoring of clinical practice through nurse coordinator rounds and outcome assessments (Figure 1).
Figure 1. PDSA cycle
PDSA-guided SBL workshops not only improved nurses’ knowledge and confidence but also provided a structured framework for continuous quality improvement in clinical education, supporting contemporary best practices in palliative nursing1,2,3,4.
Although some of the referenced literature includes hospice-specific education, the present workshop focused on general palliative care symptom management rather than exclusively end-of-life or hospice care. The educational content addressed symptom control across the continuum of serious and chronic illness, including patients with advanced but not necessarily terminal conditions. Simulation scenarios were designed to reflect common symptom management challenges encountered in home-based palliative care settings, rather than exclusively imminent end-of-life care situations.
Instruments and data collection
- Knowledge questionnaire: The 15-item knowledge questionnaire was developed based on established literature in palliative care education and symptom management, including studies on simulation-based palliative training and symptom control competencies1,2,3,4,6,7,8,9. The content was aligned with core palliative care domains such as pain management, dyspnea control, gastrointestinal symptom management, communication principles, and interdisciplinary coordination. Content and face validity were established through review by two subject-matter experts (a Clinical Nurse Specialist from Outreach Medical Services and a Nursing Instructor from HHS), which was considered adequate for preliminary validation given the educational and quality improvement focus of the study. Internal consistency was evaluated using the Kuder-Richardson Formula 20 (KR-20), which yielded a value of 0.81, indicating good reliability. Prior to implementation, the questionnaire was pilot tested with a small group of nurses (n = 10) not included in the final sample to assess clarity and feasibility, and no major modifications were required. These results support the questionnaire as a reliable instrument for assessing participants’ knowledge of palliative care symptom management.
- The Likert-scale survey consisted of five items rated on a 5-point scale (1 = strongly disagree to 5 = strongly agree), assessing symptom-specific confidence, communication, teamwork, decision-making, and overall satisfaction. Internal consistency was evaluated using Cronbach’s alpha, which was 0.88, indicating strong reliability. These findings support the survey as a reliable and appropriate instrument for assessing participants’ confidence, communication skills, and interprofessional collaboration in this educational intervention. Furthermore, two open-ended survey items were used to capture participants’ perceptions of workshop strengths and suggestions for improvement. Responses and debrief notes were reviewed and descriptively coded to identify recurring patterns and common categories. Given the limited scope of qualitative data, the analysis was exploratory and intended to provide high-level insights rather than a full thematic analysis.
- Qualitative feedback: Two open-ended items on strengths and suggestions; debrief transcripts summarized.
All assessments administered immediately pre- and post-workshop. No patient data were collected.
When compared with existing literature, the observed effect size in this study is notably strong. Previous studies of simulation-based palliative care education have generally demonstrated moderate to large improvements in knowledge and self-efficacy, with reported effect sizes commonly ranging from medium (≈0.5) to large (≈1.0), particularly among undergraduate nursing students1,2,3,4,6,7,8. In contrast, the present intervention demonstrated a very large effect (Cohen’s d > 1.5), suggesting that simulation-based learning tailored to practicing nurses within a real clinical service may produce greater educational impact. This finding supports calls in the literature for expanding simulation research beyond student populations to include in-service and postgraduate nursing education⁴.
Ethical Considerations
This study involved an educational intervention with practicing nurses and did not include patient data or interventions that could pose a risk to participants. In accordance with institutional policy for quality improvement activities, formal IRB review was not required, as the project was conducted as a quality improvement and professional development activity within the HHS unit. Participation was entirely voluntary, and all participants provided informed consent prior to data collection. Confidentiality of responses was maintained, and data were analysed in aggregate to ensure anonymity.
Results
Analysis
Pre- and post-training knowledge scores were analysed using a paired t-test, with a significance level set at p < 0.05. Descriptive statistics were used to summarize survey responses, including confidence, decision-making, teamwork, practical case discussions, and overall satisfaction.
Qualitative feedback from participants was collected through two open-ended survey items that captured perceptions of workshop strengths and suggestions for improvement. Responses and debrief notes were reviewed and descriptively coded to identify recurring patterns and common categories, generating high-level qualitative insights. Given the limited scope of qualitative data, the analysis was exploratory and not intended as a comprehensive thematic analysis. The pre-test mean score was 58.4% ± 10.6, which increased to a post-test mean of 87.3% ± 8.9, indicating a statistically significant improvement in knowledge (p < 0.001). The magnitude of knowledge improvement observed in this study is notable when compared with existing literature. Simulation-based palliative care education has consistently demonstrated moderate to large effects on knowledge and self-efficacy, with most studies reporting effect sizes ranging from approximately 0.5 to 1.0, particularly in undergraduate or pre-licensure nursing populations1,2,3,4,6,7,8. In contrast, the present study demonstrated a very large effect size (Cohen’s d > 1.5), suggesting a stronger educational impact among practicing nurses in a real-world clinical service setting.
Knowledge outcomes
Participants showed a significant improvement in knowledge scores, increasing from 58.4% ± 10.6 to 87.3% ± 8.9 (p < 0.001), indicating a 70% relative gain. Furthermore, 75% of participants reported enhanced interprofessional collaboration and decision-making based on Likert-scale feedback, highlighting the role of simulation in fostering interprofessional synergy and improving clinical decision-making in palliative care.
The pre-workshop mean score was 58.4% (SD = 10.6), and the post-workshop mean score was 87.3% (SD = 8.9), so the paired t-test showed significant improvement (t (32) = 15.92, p < 0.001). Cohen’s d indicated a large effect size (>1.5), which is a relative improvement of ≈ 70%.
Likert Scale Feedback
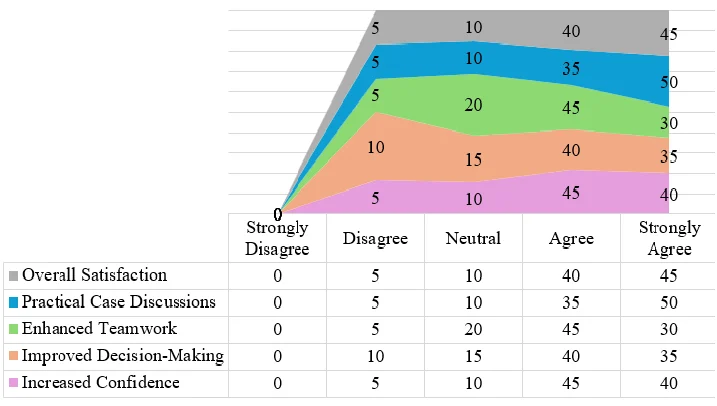
For increased confidence, 40% of participants strongly agreed and 45% agreed that the course improved their confidence. Regarding decision-making, 35% strongly agreed and 40% agreed on enhanced capabilities. Teamwork improvements were noted, with 30% strongly agreeing and 45% agreeing. Practical case discussions were particularly well-received, with 50% strongly agreeing and 35% agreeing that they contributed to learning. Overall satisfaction was high, with 45% strongly agreeing and 40% agreeing. Minimal neutral or negative responses were reported, and no participants selected “strongly disagree,” highlighting the overall effectiveness of the simulation-based training in fostering confidence, interprofessional collaboration, and practical skills in palliative care.
Figure 2. Participants’ perceptions of the workshop
Participant suggestions
Requests for more frequent sessions, inclusion of standardized patient family interactions for communication practice, and follow-up assessments at 3–6 months to evaluate retention.
Limitations
The qualitative component was limited to two open-ended survey questions and brief debrief reflections. As a result, the analysis provides high-level feedback and does not represent a comprehensive thematic understanding of participant experiences.
Discussion
The findings suggest that combining theoretical instruction with experiential learning enables nurses to manage complex patient needs confidently and provide patient-centered care. In addition to this, the observed improvement in knowledge scores represents a large effect size, which aligns with previous studies of simulation-based palliative care education reporting considerable gains in knowledge and confidence1,2,3,4,6,7,8. This comparison suggests that structured, experiential workshops can achieve similar or greater knowledge improvement in practicing nurses compared to student-focused interventions.
The practical relevance of the scenarios and the real-world context of the participants likely contributed to the observed gains. This may be attributable to the immediate clinical relevance of the scenarios, participants’ prior exposure to palliative care cases, and the integration of simulation within a PDSA-guided quality improvement framework. Unlike student-focused interventions conducted in academic settings, this workshop targeted in-service nurses responsible for direct patient care, which may have enhanced engagement, motivation, and knowledge retention. These findings extend existing evidence by demonstrating that simulation-based learning can produce equal or greater gains in postgraduate and in-service nursing populations, supporting calls to expand palliative care simulation research beyond student cohorts⁴.
This study evaluated the impact of a simulation-based workshop on nurses’ knowledge, confidence, and interprofessional collaboration in palliative symptom management within a home-based care setting. The findings demonstrate a statistically significant improvement in knowledge scores, with a very large effect size, alongside positive perceptions of enhanced confidence, teamwork, and clinical decision-making.
The substantial increase in knowledge (from 58.4% to 87.3%) suggests that integrating didactic teaching with experiential simulation can effectively address educational gaps in palliative symptom management among practicing nurses. The large effect size observed in this study exceeds those commonly reported in undergraduate simulation-based interventions6,7,8, which may be attributed to the clinical relevance of the scenarios for in-service nurses actively engaged in patient care. Adult learning theory suggests that experiential learning is particularly impactful when immediately applicable to clinical practice, which may explain the magnitude of improvement observed.
Importantly, the workshop addressed previously identified barriers to effective palliative care delivery, including limited structured training opportunities and low confidence in managing complex symptoms. By providing a psychologically safe environment for practice, simulation allowed participants to rehearse symptom assessment, medication-related decision-making, and communication strategies without risk to patients. This likely contributed not only to knowledge gains but also to enhanced perceived self-efficacy and interdisciplinary coordination.
The positive Likert-scale responses regarding teamwork and decision-making highlight the value of simulation in fostering interprofessional awareness and collaboration. In home health settings, nurses frequently function with a high degree of autonomy while maintaining communication with physicians and other team members remotely. Strengthening clinical reasoning and structured communication skills is therefore essential to ensuring safe and coordinated care.
Unlike many prior studies focused on undergraduate students or hospice-specific populations, this intervention targeted practicing nurses providing care across the continuum of serious illness. This broader palliative focus enhances the generalizability of findings to similar home-based and community care services. Furthermore, embedding the workshop within a PDSA-guided framework supports iterative refinement and sustainability, aligning educational innovation with quality improvement principles.
The qualitative feedback further supports the quantitative findings, as participants requested more frequent sessions and follow-up assessments, indicating perceived value and engagement. The request for inclusion of standardized family communication scenarios suggests an emerging need to strengthen communication training alongside symptom management competencies.
Overall, the findings support the integration of simulation-based learning into continuing professional development programs for practicing nurses. In resource-constrained healthcare settings, structured experiential education may be a practical strategy to strengthen palliative care capacity without requiring prolonged formal training programs.
Recommendations and future research
- Conduct multi-site trials and longitudinal follow-up at 3–12 months to assess retention and practice change.
- Compare simulation modalities (high-fidelity vs. standardized patient vs. hybrid) for cost-effectiveness and transfer to practice.
- Evaluate effects on patient symptom outcomes and safety metrics where feasible.
- Use PDSA cycles to iteratively refine content, frequency, and delivery modes (e.g., blended learning, spaced repetition).
Conclusion
In conclusion, a focused PDSA guided by Integrating theoretical knowledge with experiential learning equips nurses to confidently manage complex patient needs, ensuring patient-centered care. Embedding such SBL into regular continuing professional development, combined with iterative QI cycles and longitudinal assessment, has the potential to strengthen palliative care delivery and patient outcomes. To ensure sustainability, regular refresher courses and incorporation of these workshops into ongoing professional development programs are recommended. Healthcare institutions should also adopt a palliative curriculum and encourage participation to promote high-quality palliative care delivery.
Licence
© Author (s), [2026].
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, and unrestricted adaptation and reuse, including for commercial purposes, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
References
-
Condry HM, Davis L, Park M. Simulation in end-of-life nursing education: a literature review. Nurse Educ Pract. 2021;49:102907.
-
Escribano S, Belda R, Contreras A, Fernández-Méndez F, Rodríguez-Ballesteros M. Efficacy of a standardised patient simulation programme for complex chronic and end-of-life scenarios: effects on communication self-efficacy. Int J Environ Res Public Health. 2021;18(21):11673.
-
Li X, Zhang Y, Li Y, et al. The impact of virtual clinical simulation on nursing students’ palliative care knowledge, ability, and attitudes: a mixed-methods study. Nurse Educ Today. 2023;122:105670.
-
Skedsmo K, Gonçalves Nes A A, Vistven Stenseth H, Hofsø K, Hamilton Larsen M, Hilderson D, Smis D, Lundh Hagelin C, Olaussen C, Trygg Solberg M, Bingen HM, Ølnes MA, Steindal SA. Simulation‑based learning in palliative care in postgraduate nursing education: a scoping review. BMC Pall Care. 2023;22(1):30
-
Abad-Corpa E, González-Hernando A, Martínez-Cortés M, Jiménez-Ruiz I. Assessment of high-fidelity simulation with actors in palliative care training for nursing students. Nur Reports.2023;13(3).
-
Alharbi A, Nurfianti A, Mullen RF, McClure JD, Miller WH. The effectiveness of simulation-based learning on students’ knowledge and skills in nursing programs: a systematic review. BMC Med Educ. 2024;24:1099.
-
Gillan PC, Smith A, Jones R. Nursing students’ satisfaction and self-confidence with standardized patient palliative care simulation focusing on difficult conversations. Pall & Supp Care;22(5):1237-1244.
-
Son S, Min D, Kim S. Effectiveness of a simulation programme with lectures about end-of-life care using a standardised patient: a quasi-experimental study. BMC Nurs. 2025;24:371.
-
Açıl A, Keçeci A, Demiray A, Kızıltepe SK, İlaslan N, Ertürk F. The acquisition and effectiveness of “IDEAL” standards in discharge planning and education with simulation method. BMC Nursing. 2025;24:856.